J Korean Ophthalmol Soc.
2007 Oct;48(10):1312-1317. 10.3341/jkos.2007.48.10.1312.
Treatment of Distichiasis or Trichiasis combined with Entropion
- Affiliations
-
- 1Department of Ophthalmology, Cheil Eye Hospital, Daegu, Korea. healeye@nate.com
- KMID: 2210982
- DOI: http://doi.org/10.3341/jkos.2007.48.10.1312
Abstract
-
PURPOSE: To evaluate the clinical efficacy of a reverse eyelid splitting technique that we performed in cases of trichiasis or distichiasis combined with entropion.
METHODS
The study comprised 43 eyes of 31 patients with trichiasis or distichiasis combined with entropion treated from November 2004 to December 2005. After skin incision, the muscular layer and tarsus were reversely dissected to find abnormal follicles. The abnormal hair follicle was cauterized under the muscular layer, and 2~3 rotating sutures were done with Ethilon 6-0 to fix the tarsus and skin. Success was defined as having the meibomian gland located in front of the junction of skin and mucosa, without an abnormal hair protruding into the eye for at least three months.
RESULTS
Fifteen patients were male and sixteen patients were female. The mean age was 62.1+/-15.2 years. The patients were followed up for an average of 12.4+/-2.0 months after surgery. Surgery was successful in 74.4% (32 of the 43 eyelids) of the cases, and the recurrence rate was 25.6% (11 of the 43 eyelids). No severe complications occurred, such as infection, hemorrhage, wound dehiscence, or granuloma. However, foreign body sensation (1 eye) and eyelid notch (l eye) did occur.
CONCLUSIONS
This reverse eyelid splitting technique produced satisfactory results in both cosmetic and functional aspects. Moreover, it resulted in a low recurrence rate and low complication rate in patients with trichiasis or distichiasis combined with entropion.
Keyword
MeSH Terms
Figure
-
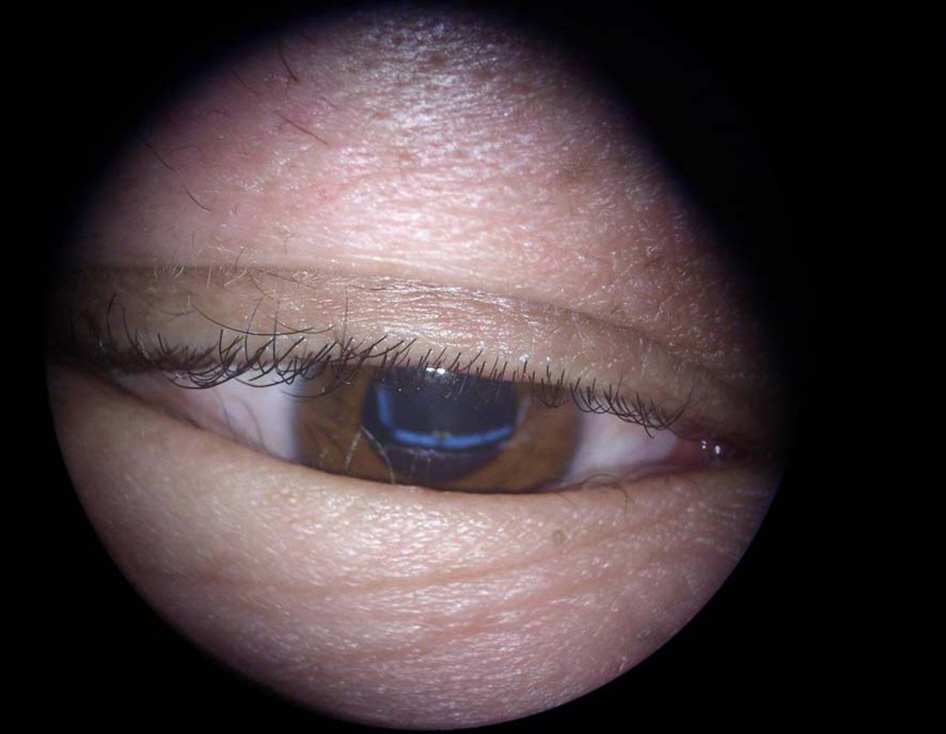
Figure 1. Preoperative view. The lower eyelid was inverted and cilia touched the cornea.

Figure 2. With the lower lid skin being pulled down, incision lines were designed.
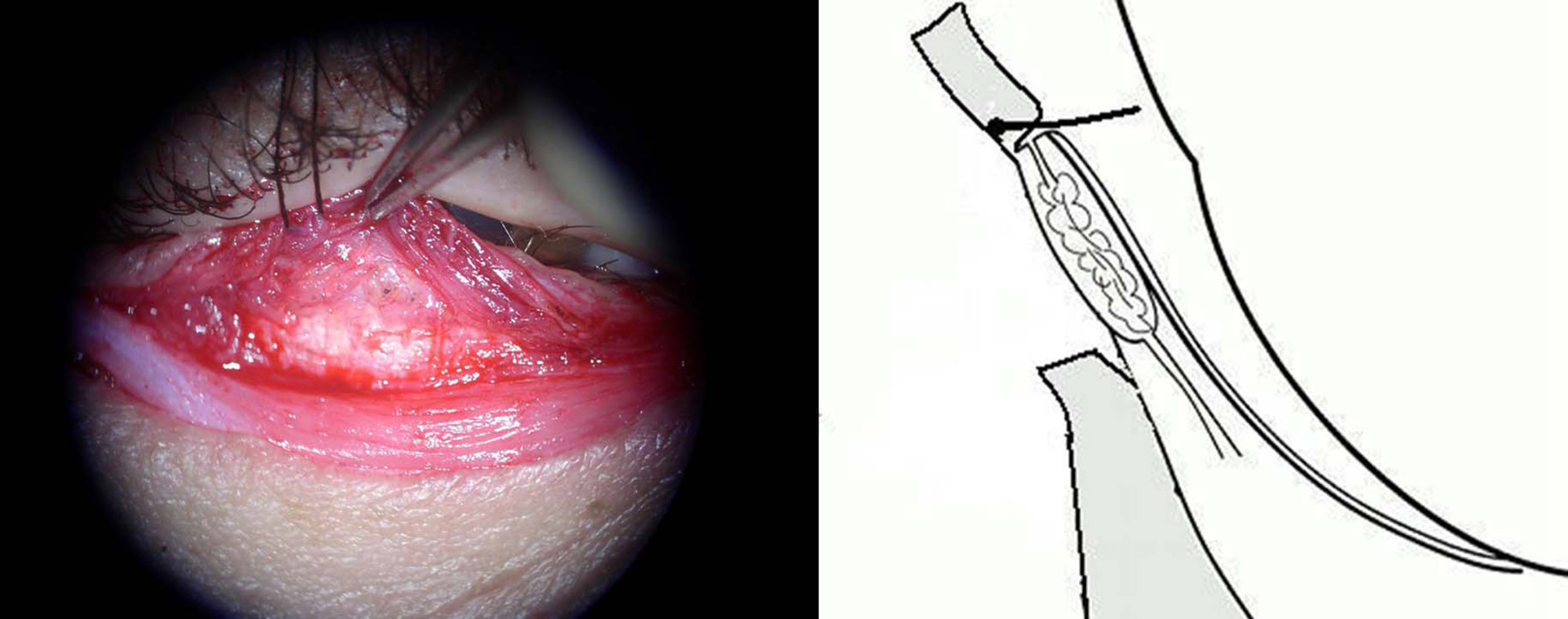
Figure 3. After excision of excessive skin and muscle layer, remaining muscle layer and tarsal plate were dissected.

Figure 4. Cauterization was done at the point of abnormal hair follicles.

Figure 5. After rotating suture with Ethilon 6-0, meibomian glands were repositioned to normal posiotion.

Figure 6. Skin suture was done by a Black silk 6-0. The eyelid was everted, and no cilia touched the cornea.
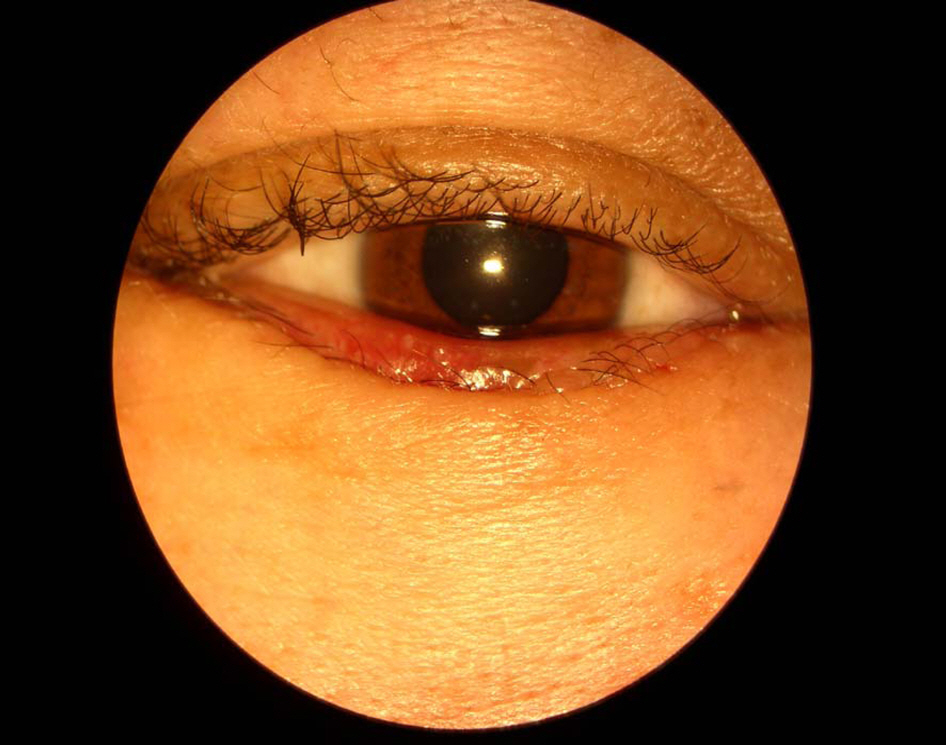
Figure 7. Postoperative 7th-day view. Meibomian glands were repositioned to normal position and no cilia touched the cornea.
Reference
-
References
1. Kim YD, Ku HJ, Yi KY, Kim TW. Surgical correction of epiblepharon. J Korean Ophthalmol Soc. 1998; 39:11–5.2. Baek SH, Bae JY. The effect of single suture inferior retractor tightening for the effect of single suture inferior retractor tightening for senile entropion. J Korean Ophthalmol Soc. 2004; 45:1215–20.3. Park DW, Kim YD. Eyelid splitting and microsurgical excision for congenital distichiasis. J Korean Ophthalmol Soc. 1999; 40:2657–61.4. Vaughn GL, Dortzbach RK, Sires BS, Lemke BN. Eyelid splitting with excision or microhyfrecation for distichiasis. Arch Ophthalmol. 1997; 115:282–4.
Article5. Chi MJ, Park MS, Nam DH, et al. Eyelid splitting with follicular extirpation using a monopolar cautery for the treatment of trichiasis and distichiasis. Graefes Arch Clin Exp Ophthalmol. 2005; 17:1–4.
Article6. Wolfley D. Excision of individual follicles for the management of congenital distichiasis and localized trichiasis. J Pediatr Ophthalmol Strabismus. 1987; 24:22–6.
Article7. O'Donnell BA, Collin JR. Distichiasis: management with cryotherapy to the posterior lamella. Br J Ophthalmol. 1993; 77:289–92.8. An HB, Ha SU, Lee DW. A clinical effects between Ellman Surgitron thermolysis and argon laser thermoablation in trichiasis. J Korean Ophthalmol Soc. 2003; 44:2191–6.9. Anderson RL, Harvey JT. Lid splitting and posterior lamella cryosurgery for congenital and acquired distichiasis. Arch Ophthalmol. 1981; 99:631–4.
Article10. Bosniak S. Principles and practice of ophthalmic plastic and reconstructive surgery. 1st ed.Philadelphia: WB Saunders company;1996. p. 774–5.11. Dortzbach RK. Ophthalmic Plastic Surgery. 1st ed.New York: Raven press;1994. p. 42–8.12. Seiff SR, Carter SR, Tovilla Y, et al. Tarsal margin rotation with posterior lamella supraadvancement for the management of cicatricial entropion of the upper eyelid. Am J Ophthalmol. 1999; 127:67–71.13. Rosner M, Bourla N, Rosen N. Eyelid splitting and extirpation of hair follicles using a radiosurgical technique for treatment of trichiasis. Ophthalmic Surg Lasers Imaging. 2004; 35:116–22.
Article14. Long JA, Goldberg RA. Entropion. In : Bosniak S, editor. Principles and practice of ophthalmic plastic and reconstructive surgery. 1st ed.Philadelphia: WB Saunders company;1996. v. 1. chap. 38.15. Wies FA. Surgical treatment of entropion. J Int Coll Surg. 1954; 21:758–60.16. Tenzel RR. Repair of entropion of upper lid. Arch Ophthalmol. 1967; 77:675.
Article17. Kim SA, Rho JH. Tarsal margin rotation with blepharoplasty to correct cicatricial entropion of the upper eyelid. J Korean Ophthalmol Soc. 2005; 46:196–200.18. Wojno TH. Lid splitting with lash resection for cicatricial entropion and trichiasis. Ophthal Plast Reconstr Surg. 1992; 8:287–9.
Article19. Sodhi PK, Yadava U, Pandey RM, Mehta DK. Modified grey line split with anterior lamellar repositioning for treatment of cicatricial lid entropion. Ophthalmic Surg Lasers. 2002; 33:169–74.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical experience in marginal rotation
- Effect of Full-thickness Pentagonal Wedge Resection for Treatment of Localized Trichiasis and Distichiasis
- Correction of the Trichiasis and the Cicatricial Entropion by Transposition of Skin Flaps
- New Operation Method on the Cicatricial Entropion and the Distichiasis
- The Effectiveness of Partial Lid Margin Excision Including Hair Follicles in Diffuse Trichiasis and Distichiasis
