Analysis of Aortic Passage in the Thoracic Region by Magnetic Resonance Imaging
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea. schsbj@schbc.ac.kr
- KMID: 2209710
- DOI: http://doi.org/10.4184/jkss.2002.9.4.289
Abstract
-
STUDY DESIGN: The relationships between aorta and thoracic vertebrae were analyzed by using MR images.
OBJECTIVES
The purpose of this study was to provide information upon the thoracic aortic passage to prevent vascular compli-cations during anterior and posterior instrumentations for various spinal disorders and traumas. SUMMARY OF BACKGROUND DATA: A number of morphometric investigations have been performed on the thoracic vertebrae, but the anatomical relationship between aorta and the thoracic vertebral body has not been analyzed.
METHODS
The MR images of 32 patients with normal thoracic vertebral column were obtained. The angle between the transverse axis of the thoracic vertebral body and the thoracic aorta, the diameter of the thoracic aorta and the closest distance between the thoracic vertebral body and the thoracic aorta from T2 to T12 were measured on axial MR images.
RESULTS
The smallest angle between the transverse axis of the thoracic vertebral body and the line connecting the centers of the vertebral body and aorta was 6.8 degrees/3.7 degrees(male/female) in the T5-6 region and highest angle observed was 56.3 degrees/55 degrees in the T12 region. The angle decreased between T2 and T5-6 and then increased after T6. The mean external diameter of the thoracic aorta was 32.8 mm, and the largest diameter of the thoracic aorta was 24.7/25.4 mm (M/F) in the T4-5 region. The aortic arch was first seen in the T2 region and it formed an arch in the T3-4 region. The shortest distance between the thoracic vertebral body and the thoracic aorta wall was 0.8/0.7 mm in the T12 region and the greatest distance between the vertebral body and the aorta was 11.84/6.75 mm in the T2-3 region.
CONCLUSION
From T4 to T8, the aorta is located just left lateral to the vertebral body. In this area, the aorta is jeopardized by a screw penetrating the vertebral body during anterior instrumentation, if the screw protrudes beyond the pedicle during posterior instrumentation. The surgeon should be familiar with the anatomical relationship between aorta and the vertebral column when planning a surgical procedure or the use of instrumentation in this region.
MeSH Terms
Figure
-
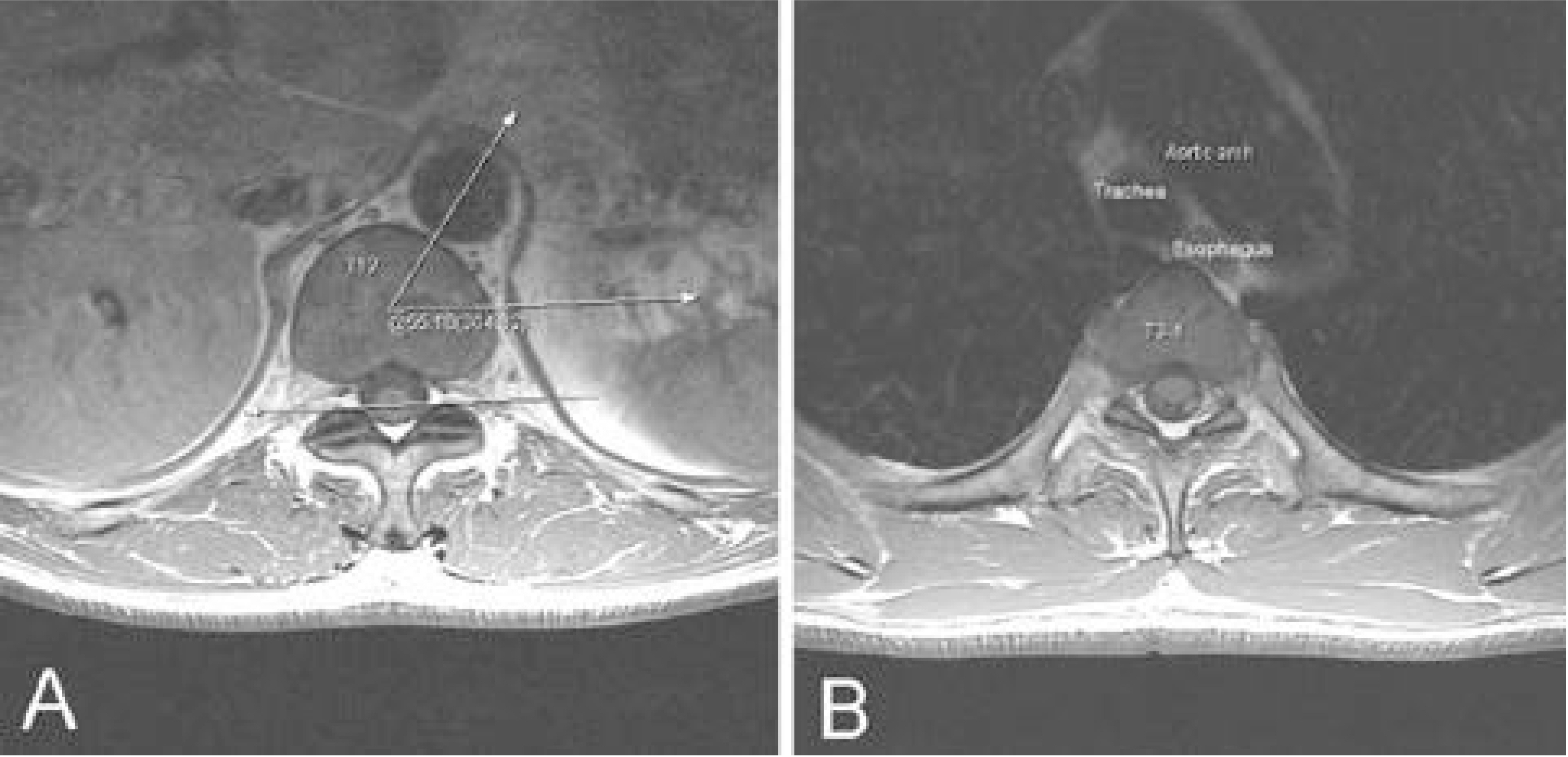
Fig. 1. Angle measurement for describing relationship between vertebral body and aorta in axial MR images. Fig. 1. A. Angle between the transverse axis of the vertebral body and the line connecting centers of the vertebral body and aorta is measured by angle tool of PiView program. (Transverse axis of vertebral body is drawn parallel to the line connecting the both anterior margin of posterior facet. The axis also passes the center of vertebral body.) A maximal angle is obtained at T12 level. Fig. 1. B. Aortic arch was first seen at the level of T2 and form arch at T3-4 level.
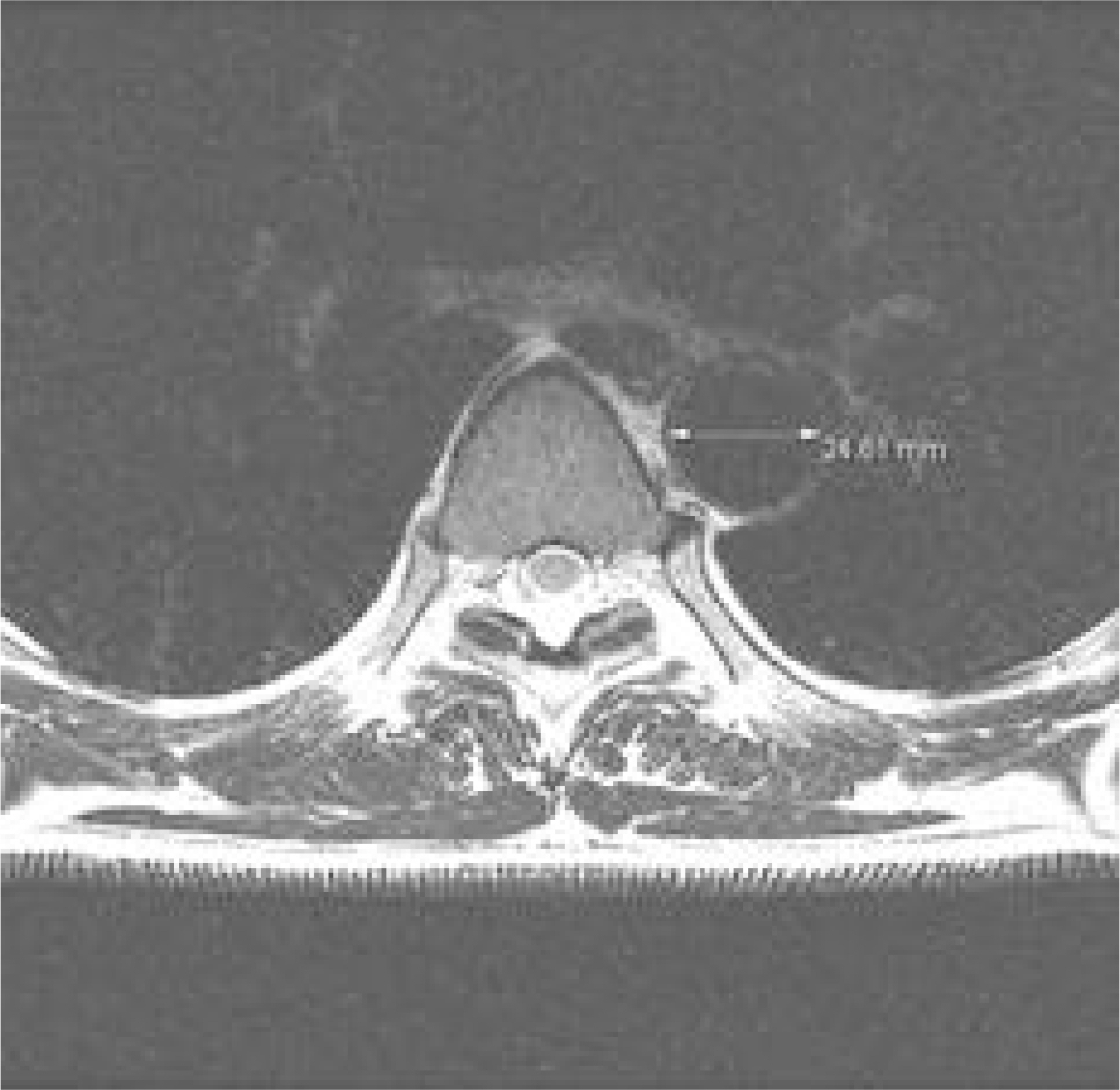
Fig. 2. Diameter of thoracic aorta at T4-5 level.

Fig. 3. A. The shortest distance between vertebral body and aorta at T12 level. Fig. 3. B. The longest distance between vertebral body and aorta at T2-3 level.
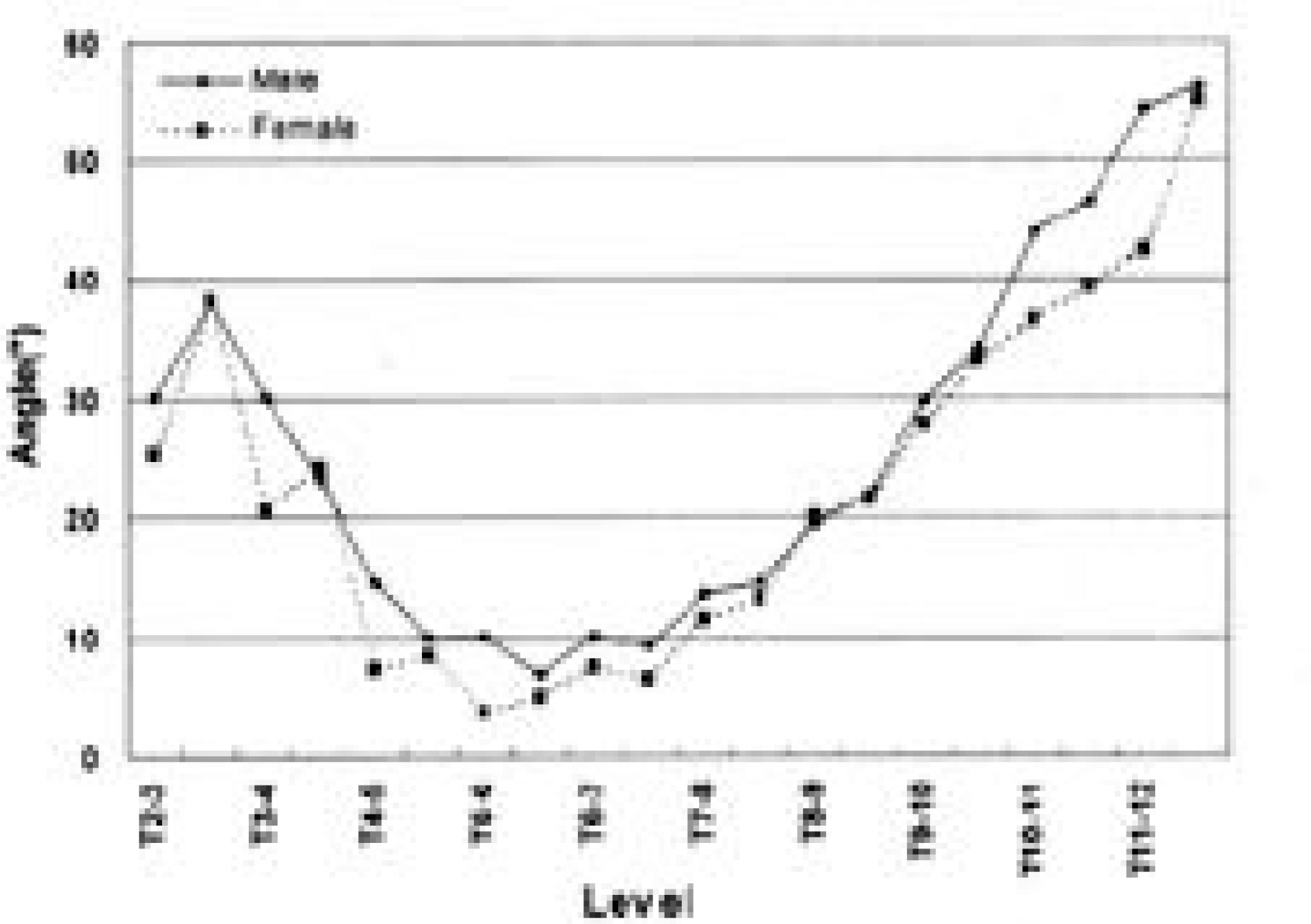
Fig. 4. Graph showing the variation of angles between the transverse axis of thoracic vertebral body and thoracic aorta(°).
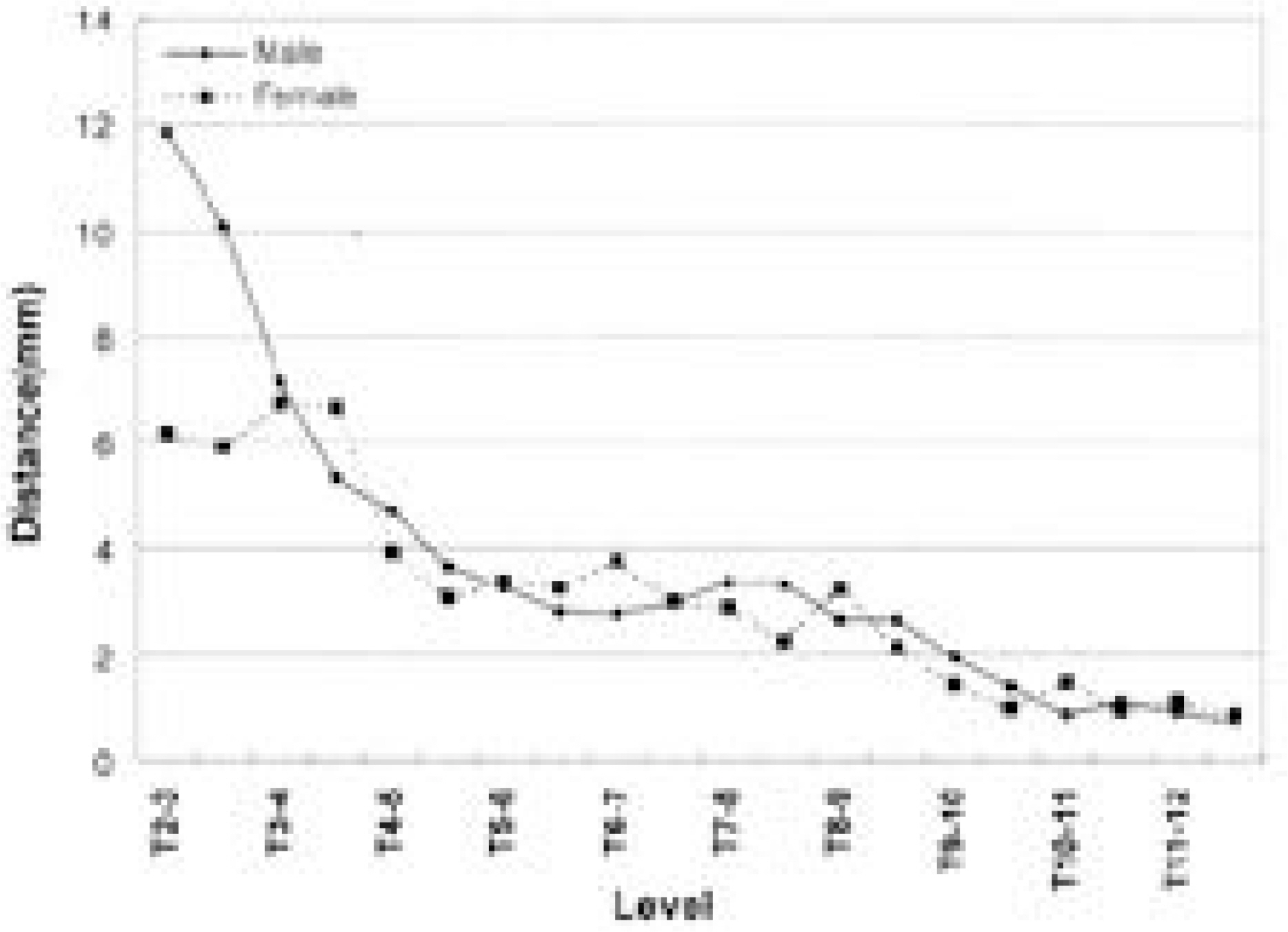
Fig. 5. Changes of distance between vertebral body and aorta
Reference
-
1). Davne SH and Myers DL. Complication of lumbar spine fusion with transpedicular instrumentation. Spine. 17:184–189. 1992.2). Link KM, Loehr SP, Baker DM and Lesko NM. Magnetic resonance imaging of the thoracic aorta. Semin Ultrasound CT MR. 14-2:91–105. 1993.
Article3). McAfee PC, Weiland DJ and Carlow JJ. Survivorship analysis of pedicle spinal instrumentation. Spine. 16:422–427. 1991.
Article4). Roy-camile R, Saillant G and Mazel C. Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop. 203:7–17. 1986.5). Suk Se-Il. Spinal Surgery. 1st ed. Seoul: Cheishin medical pub;p. 1–31. 1997.6). West JL, Ogilvie JW and Bradford DS. Complication of the variable screw plate pedicle screw fixation. Spine. 16:576–579. 1990.7). Whitecloud TS, Butler JC, Cohen JL and Candelora PD. Complication with the variable spinal plating system. Spine. 14:472–476. 1988.8). Whitecloud TS, Skalley TC, Cook SD and Morgan EL. Roentgenographic measurement of pedicle screw pene -tration. Clin Orthop. 245:57–68. 1989.9). Zindrick MR. The role of transpedicular fixation system for stabilization of the lumbar spine. Orthop Clin North AM. 22:333–44. 1991.10). Zindrick MR, Wiltse LL, Widell EH, Thomas JC, Hol-land WR and Spencer CW. A biomechanical study of intrapedicular screw fixation in the lumbar spine. Clin Orthop. 203:99–112. 1986.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Undifferentiated Pleomorphic Sarcoma of the Descending Thoracic Aorta Mimicking Pseudoaneurysm with Periaortic Hematoma: a Case Report
- Magnetic resonance imaging in thoracic disease
- Imaging Study of Diseases of the Aorta
- MR Imaging Findings of Traumatic Thoracic Aortic Injury
- Coarctation of the Aorta Associated with Chronic Thoracic Aortic Aneurysm: A case report
