Recompression of Vertebral Bodies after Balloon Kyphoplasty for Vertebral Compression Fractures : Preliminary Report
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, The Catholic University of Korea. kwrhyu@catholic.ac.kr
- KMID: 2209602
- DOI: http://doi.org/10.4184/jkss.2009.16.2.89
Abstract
-
STUDY DESIGN: This is a retrospective and preliminary study.
OBJECTIVES
We wanted to evaluate the characteristics of recompression of vertebral bodies without trauma after balloon kyphoplasty (KP) for treating osteoporotic vertebral compression fractures (VCF). SUMMARY OF THE LITERATURE REVIEW: KP has been used for fracture reduction, maintenance of vertebral height and relief of pain in VCF. Despite of numerous satisfactory results, several factors have been noted to affect the clinical results of KP.
MATERIALS AND METHODS
Six patients with recompression of vertebral bodies without trauma after KP were reviewed. All the patients were female and their mean age was 75.9+/-4.1 years old. The follow-up period was 17.2+/-8.5 months. The compression rates of the operated vertebral bodies (CR) and the kyphotic angles (KA) were checked by using plain roentgenograms at the initial, postoperative and last follow-up periods. The preoperative MRIs were also reviewed. The clinical results were checked using the VAS.
RESULTS
The CRs at the initial, postoperative and last follow-up periods were 33.7+/-14.8%, 13.4+/-7.6% and, 26.9+/- 9.9%, respectively. The KAs were 19.2+/-7.2degrees , 14.8+/-6.2degrees and 20.5+/-7.4degrees for each period, respectively. Statistically, the CR and KA at the initial-postoperative period and at the postoperative-last follow-up period showed significant differences (p < 0.05). Intervertebral clefts were found in all the cases on MRI. Normal bones superior or inferior to cement were also seen in all the cases after KP. The VAS scores were 8.5+/-0.5, 2.3+/-0.5 and 3.0+/-0.6, retrospectively, and there were significant differences between each periods (p<0.05).
CONCLUSIONS
Recompression of a vertebral body without trauma after KP for treating VCF was observed in the cases with a intervertebral cleft seen on MRI and normal bones superior or inferior to the cement were observed after KP. The causes of recompression may be subsequent compression or resorption of the remaining vertebral body.
Keyword
Figure
-
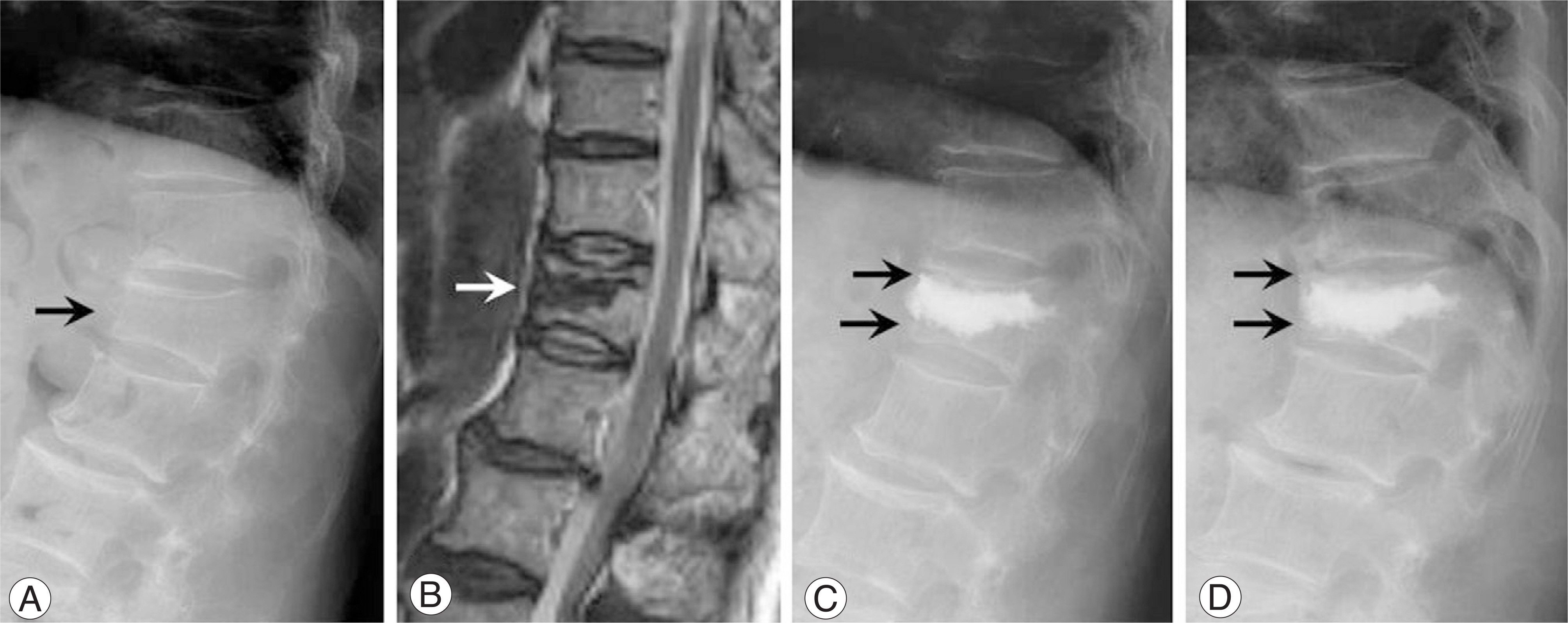
Fig. 1. 81 years-old female with D12 vertebral compression fracture (case 6). (A) Initial plain roentgenogram. The initial height loss was 34.5% and initial T-score was -4. Initial kyphotic angle was 31。 (black arrow). (B) The T2-weighted MRI image showed the intervertebral cleft (white arrow). (C) The balloon kyphoplasty was done and the fracture was reduced into 13.8% of body compression and 26。 of kyphotic angle. The normal portions of vertebral body were seen at superior and inferior aspect of the cement (black arrows) after surgery. (D) The plain roentgenogram showed resorption of the remained vertebral body at 14 months after the surgery (black arrows). The inferior portion of vertebral body was resolved mainly. Body compression rate was increased into 31% and the kyphotic angle was resulted to 33。. The initial, postoperative, and last VAS score were 9, 2 and 2, retrospectively.
Cited by 1 articles
-
Vertebral Recompression after Vertebroplasty or Kyphoplasty
Deuk Soo Jun, Do Hyun Moon, Young Kyu Ko, Jang Seok Choi, Byoung Keun An, Je Won Paik, Min Ho Park
J Korean Fract Soc. 2015;28(2):110-117. doi: 10.12671/jkfs.2015.28.2.110.
Reference
-
1). Lieberman IH, Dudeney S, Reinhardt MK, et al. .:. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001; 26:1631–1638.
Article2). Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine. 2001; 26:1511–1515.3). Lieberman I, Reinhardt MK. Vertebroplasty and kyphoplasty for osteolytic vertebral collapse. Clin Orthop Relat Res. 2003; 415:176–186.
Article4). Voggenreiter G. Balloon kyphoplasty is effective in deformity correction of osteoporotic vertebral compression fractures. Spine. 2005; 30:2806–2812.
Article5). Garfin SR, Buckley RA, Ledlie J, et al. .:. Balloon kyphoplasty for symptomatic vertebral body compression fractures results in rapid, significant, and sustained improvements in back pain, function, and quality of life for elderly patients. Spine. 2006; 31:2213–2220.
Article6). Taylor RS, Fritzell P, Taylor RJ. Balloon kyphoplasty in the management of vertebral compression fractures: an updated systematic review and meta-analysis. Eur Spine J. 2007; 16:1085–1100.
Article7). Lindsay R, Silverman SL, Cooper C, et al. .:. Risk of new vertebral fracture in the year following a fracture. JAMA. 2001; 285:320–323.
Article8). Kanis J, Johnell O, Oden A, et al. .:. The risk and burden of vertebral fractures in Sweden. Osteoporos Int. 2004; 15:20–26.
Article9). Belkoff SM, Mathis JM, Fenton DC, et al. .:. An ex vivo biomechanical evaluation of an inflatable bone tamp used in the treatment of compression fracture. Spine. 2001; 26:151–156.
Article10). Polikeit A, Nolte LP, Ferguson SJ. The effect of cement augmentation on the load transfer in an osteoporotic functional spinal unit: finite element analysis. Spine. 2003; 28:991–996.11). Berlemann U, Ferguson SJ, Nolte LP, et al. .:. Adjacent vertebral failure after vertebroplasty: a biomechanical investigation. J Bone Joint Surg Br. 2002; 84:748–752.12). Fribourg D, Tang C, Sra P, et al. .:. Incidence of subsequent vertebral fracture after kyphoplasty. Spine. 2004; 29:2270–2276.
Article13). Harrop J, Prpa B, Reinhardt M, et al. .:. Primary and secondary osteoporosis incidence of subsequent vertebral compression fractures after kyphoplasty. Spine. 2004; 29:2120–2125.
Article14). Lavelle WF, Cheney R. Recurrent fracture after vertebral kyphoplasty. Spine J. 2006; 6:488–493.
Article15). Maldague BE, Noel HM, Malghem JJ. The intravertebral vacuum cleft: a sign of ischemic vertebral collapse. Radiology. 1978; 129:23–29.
Article16). Sta¨bler A, Schneider P, Link TM, et al. .:. Intravertebral vacuum phenomenon following fractures: CT study on frequency and etiology. J Comput Assist Tomogr. 1999; 23:976–980.17). Naul LG, Peet GJ, Maupin WB. Avascular necrosis of the vertebral body: MR imaging. Radiology. 1989; 172:219–222.
Article18). Laloux P, Lefebvre S, Esselinckx W, et al. .:. Spinal cord compression secondary to vertebral aseptic osteonecrosis. Spine. 1991; 16:480–481.19). Dupuy DE, Palmer WE, Rosenthal DI. Vertebral fluid collection associated with vertebral collapse. AJR Am J Roentgenol. 1996; 167:1535–1538.
Article20). Chou LH, Knight RQ. Idiopathic avascular necrosis of a vertebral body. Case report and literature review. Spine. 1997; 22:1928–1932.21). Libicher M, Appelt A, Berger I, et al. .:. The intravertebral vacuum phenomen as specific sign of osteonecrosis in vertebral compression fractures: results from a radiological and histological study. Eur Radiol. 2007; 17:2248–2252.
Article22). Baba H, Maezawa Y, Kamitani K, et al. .:. Osteoporotic vertebral collapse with late neurological complications. Paraplegia. 1995; 33:281–289.
Article23). Hasegawa K, Homma T, Uchiyama S, et al. .:. Vertebral pseudarthrosis in the osteoporotic spine. Spine. 1998; 23:2201–2206.
Article24). Mochida J, Toh E, Chiba M, et al. .:. Treatment of osteoporotic late collapse of a vertebral body of thoracic and lumbar spine. J Spinal Disord. 2001; 14:393–398.
Article25). Baur A, St ¨abler A, Arbogast S, et al. .:. Acute osteoporotic and neoplastic vertebral compression fractures; fluid sign at MR imaging. Radiology. 2002; 225:730–735.
Article26). Ito Y, Hasegawa Y, Toda K, et al. .:. Pathogenesis and diagnosis of delayed vertebral collapse resulting from osteoporotic spinal fracture. Spine J. 2002; 2:101–106.
Article27). Kim MJ, Lindsey DP, Hannibal M, et al. .:. Vertebroplasty versus kyphoplasty: biomechanical behavior under repetitive loading conditions. Spine. 2006; 31:2079–2084.
Article28). Wilke HJ, Mehnert U, Claes LE, et al. .:. Biomechanical evaluation of vertebroplasty and kyphoplasty with polymethyl methacrylate or calcium phosphate cement under cyclic loading. Spine. 2006; 31:2934–2941.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of the Cement Distribution Pattern and Other Risk Factors that Affect the Incidence of Recompression Fractures of Vertebral Bodies after Vertebroplasty or Kyphoplasty
- Vertebral Recompression after Vertebroplasty or Kyphoplasty
- Single-Balloon Kyphoplasty in Osteoporotic Vertebral Compression Fractures : Far-Lateral Extrapedicular Approach
- The Factors that Affect the Deformity Correction of Vertebral Body during Kyphoplasty of Osteoporotic Vertebral Compression Fracture
- Percutaneous Pediculoplasty and Balloon Kyphoplasty in a Vertebral Metastatic Cancer Patient: A case report
