Comparison of Mechanical Property of Conventional Rods versus Growing Rods for Pediatric Early Onset Scoliosis
- Affiliations
-
- 1Department of Orthopedic Surgery, Yonsei University College of Medicine, Seoul, Korea. HAKSUNKIM@yuhs.ac
- KMID: 2209580
- DOI: http://doi.org/10.4184/jkss.2010.17.4.177
Abstract
- STUDY DESIGN: This is a mechanical study.
OBJECTIVES
We wanted to investigate the mechanical properties of newly developed dual growing rods for obtaining approval for their clinical application. SUMMARY OF LITERATURE REVIEW: The current expandable spinal implant system appears effective for controlling progressive early onset scoliosis, and it allows for spinal growth and improving lung development.
MATERIALS AND METHODS
We investigate the yield load and ultimate load during compression, tension and torsion of the growing rods and the conventional rods assembly using UHMWPE blocks, and the diameter of the rods was 6.0 mm and they expanded 5cm long. We also performed a fatigue test with growing rods, and the diameter of which was 6.0 mm and it expanded 2.5cm long. The guideline for the American Society for Testing Materials was followed during the entire mechanical test. With the growing rods and conventional rods, we tested for each mechanical property7 times with the new rods and blocks.
RESULTS
The yield load of the growing rods and conventional rods were 845.2+/-18.2 (N) and 812.9+/-29.9 (N), respectively, and the ultimate load of the growing rods and conventional rods were 961.9+/-31.1 (N) and 914.9+/-25.6 (N), respectively, when compression force was applied. The yield load and ultimate load of the growing rods were statistically higher than those of the conventional rods (p<0.05). The ultimate load of the growing rods and conventional rods were 3281.7+/-41.5 (N) and 3678.5+/-447.9 (N), respectively when tension force was applied. The ultimate load was similar for both types of rods (p>0.05). The yield loads of the growing rods and conventional rods were 11.56+/-0.59 (Nm) and 12.46+/-0.71 (Nm), respectively, the ultimate loads of the growing rods and conventional rods were 16.97+/-0.94 (Nm) and 17.42+/-2.66 (Nm) during the torsion, respectively. The yield load and ultimate load of the growing rods were statistically lower than that of the conventional rods (p<0.05).
CONCLUSIONS
The newly developed growing rods have a higher yield load and ultimate load under compression, a similar ultimate load under tension and a lower yield load and ultimate load under torsion. The differences of the yield load and ultimate load under torsion were minimal, and so the growing rods and conventional rods have similar mechanical properties.
Keyword
Figure
-
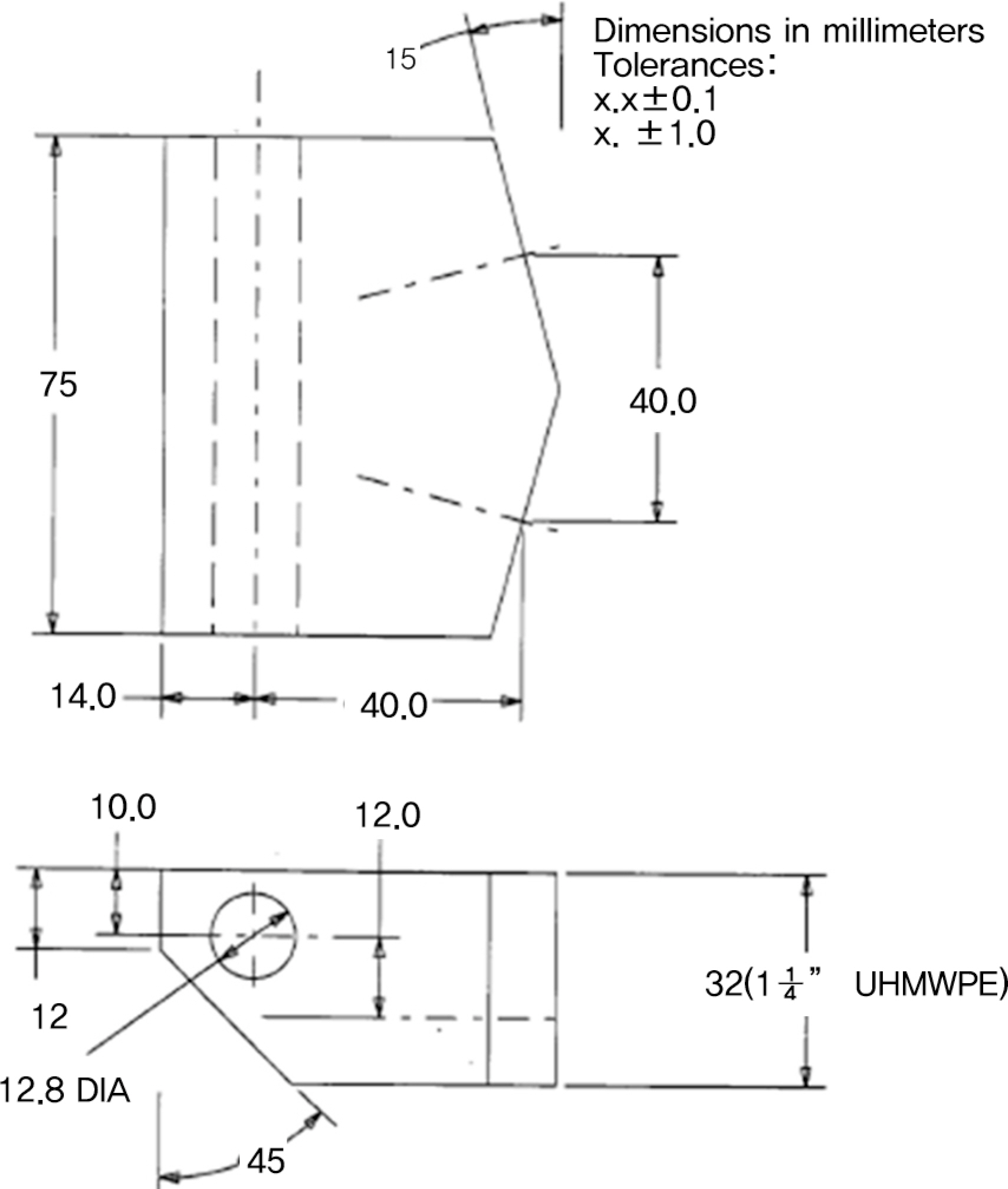
Fig.1. This picture show the standard dimension of test block follows the standards of The American Society for Testing Materials (ASTM) F1717-04.

Fig. 2These pictures show the basic assembly of the growing rods for static test (A), the growing rods for fatigue test (B) and the conventional rods for static test (C) with UHMWPE(Ultra-High Molecular Weight Polyethylene) blocks through the mechanical testing and this setup follows the standards of The American Society for Testing Materials (ASTM) F1717-04.
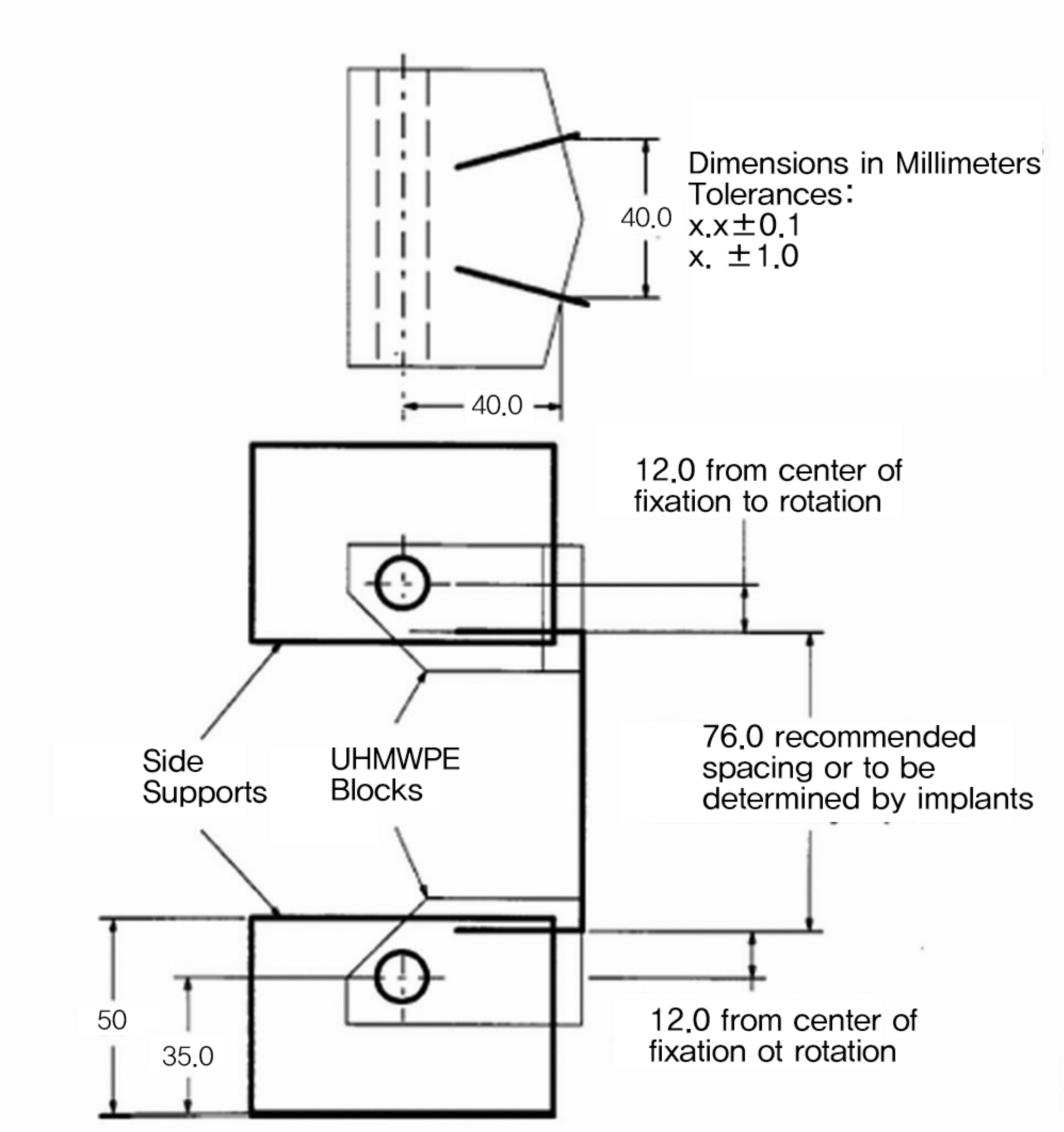
Fig. 3. These pictures show the bilateral construct test setup for screws and rods.

Fig. 4. These pictures show the test results of growing rods construct during the extension test (A), the compression test (B), and the torsion test(C).
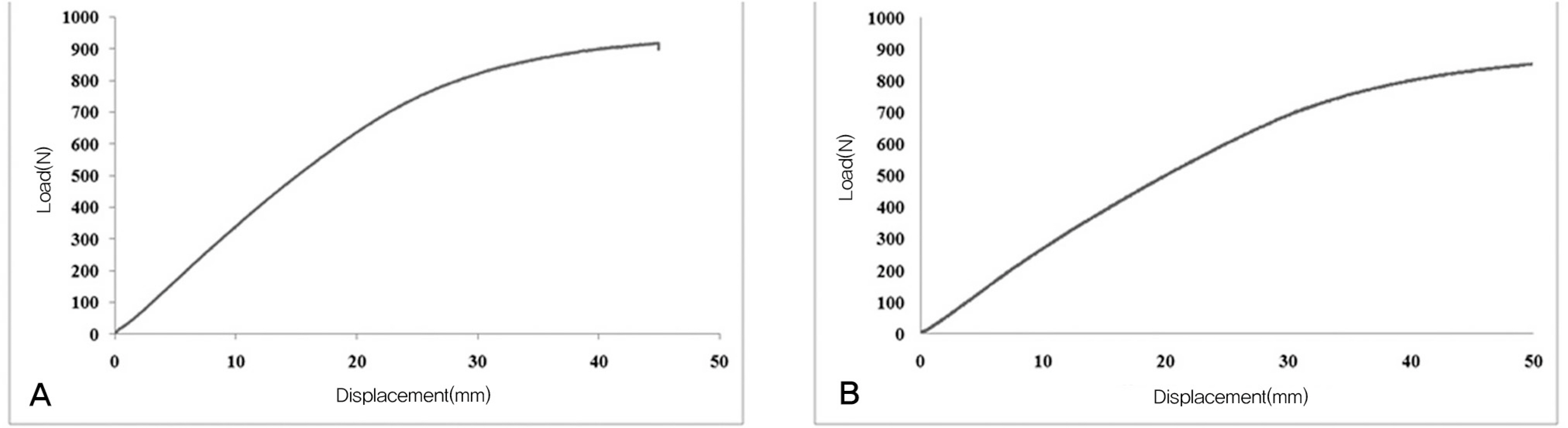
Fig. 5. These diagrams show load – displacement curve of the growing rods (A) and the conventional rods (B) during compression test.
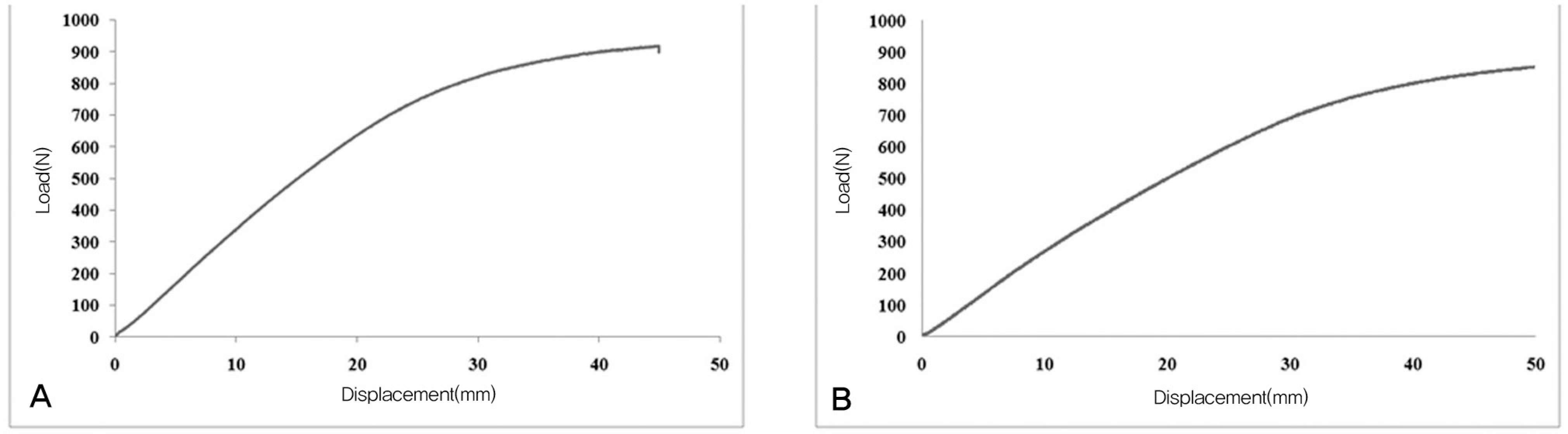
Fig. 6. These diagrams show load – displacement curve of the growing rods (A) and the conventional rods (B) during extension test.

Fig. 7. These diagrams show torque – angular curve of the growing rods (A) and the conventional rods (B) during torsion test.
Cited by 1 articles
-
Results of Dual Growing Rods Treatment for Progressive Pediatric Spinal Deformity
Hyoung Bok Kim, Hyon-Su Chong, Eun Su Moon, Hwan Mo Lee, Seong Hwan Moon, Jin Oh Park, Jea Ho Yang, Hak-Sun Kim
J Korean Soc Spine Surg. 2013;20(1):8-15. doi: 10.4184/JKSS.2021.20.1.8.
Reference
-
1.Branthwaite MA. Cardiorespiratory consequences of un-fused idiopathic scoliosis. Br J Dis Chest. 1986. 80:360–9.
Article2.Campbell RM., Smith MD., Mayes TC, et al. The charac-teristics of thoracic insufficiency syndrome associated with fused ribs and congenital scoliosis. J Bone Joint Surg Am. 2003. 85:399–408.
Article3.Mehta M., Morel G., �orab P., Siezler D. The Non-�per- ative Treatment of Infantile Idiopathic Scoliosis. London: Academic Press;1979.4.Kennedy JD., Robertson CF., �linsky A., Dickens DR., Phelan PD. Pulmonary restrictive effect of bracing in mild idiopathic scoliosis. Thorax. 1987. 42:959–61.
Article5.Klemme WR., Denis F., Winter RB., Lonstein JW., Koop SE. Spinal instrumentation without fusion for progressive scoliosis in young children. J Pediatr �rthop. 1997. 17:734–42.
Article6.Harrington PR. Treatment of scoliosis. Correction and inter-nal fixation by spine instrumentation. J Bone Joint Surg Am. 1962. 44:591–610.7.Moe JH., Kharrat K., Winter RB., Cummine JL. Harrington instrumentation without fusion plus external orthotic sup-port for the treatment of difficult curvature problems in young children. Clin �rthop Relat Res. 1984. 185:35–45.
Article8.Sengupta D., Freeman B., Grevitt M, et al. Long term follow-up of Luque trolley growing-rod construct in the surgical treatment of early onset idiopathic scoliosis. Scoliosis Research Society Annual Meeting. Seattle. 2002.9.Tello C., Bersusky E., Francheri A, et al. Severe infantile scoliosis treated with repetitive distractions followed by definitive arthrodesis. Scoliosis Research Society Annual Meeting. Seattle. 2002.10.Dubousset J., Herring JA., Shufflebarger H. The crankshaft phenomenon. J Pediatr �rthop. 1989. 9:541–50.
Article11.Roberto RF., Lonstein JE., Winter RB., Denis F. Curve pro- gression in Risser stage 0 or 1 patients after posterior spinal fusion for idiopathic scoliosis. J Pediatr �rthop. 1997. 17:718–25.12.Marchetti PG., Faldini A. End fusions in the treatment of some progressing or severe scoliosis in childhood or early adolescence. Scoliosis Research Society, 1977. �rthop Trans. 1978. 2:271.13.Mardjetko SM., Hammerberg KW., Lubicky JP., Fister JS. The Luque trolley revisited: review of nine cases requiring revision. Spine. 1992. 17:582–9.14.Rinsky LA., Gamble JG., Bleck EE. Segmental instrumentation without fusion in children with progressive scoliosis. J Pediatr �rthop. 1985. 5:687–90.15.Campbell RM., Smith M., Hell-Vocke A. Expansion tho- racoplasty: the surgical technique of opening-wedge thoracostomy. surgical technique. J Bone Joint Surg Am. 2004. 86:51–64.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimum 2-Year Experience with Magnetically Controlled Growing Rods for the Treatment of Early-Onset Scoliosis: A Systematic Review
- Results of Magnetically Controlled Growing Rods for Early Onset Scoliosis
- Results of Dual Growing Rods Treatment for Progressive Pediatric Spinal Deformity
- Traditional Dual Growing Rods With 2 Different Apical Control Techniques in the Treatment of Early-Onset Scoliosis
- Choice of Rods in Surgical Treatment of Adolescent Idiopathic Scoliosis: What Are the Clinical Implications of Biomechanical Properties? – A Review of the Literature
