T-configured Dual Stent Placement in Malignant Biliary Hilar Obstruction: Technique and Clinical Application
- Affiliations
-
- 1Department of Radiology, Konyang University Hospital, Korea.
- 2Department of Radiology, Integrated Cancer Center, Sam Anyang Hospital, Korea. radol@unitel.co.kr
- KMID: 2208915
- DOI: http://doi.org/10.3348/jksr.2010.62.3.211
Abstract
-
PURPOSE: To evaluate implanting techniques of T-configured dual stents in malignant hilar obstruction and investigate the clinical factors related to stent obstruction.
MATERIALS AND METHODS
The study included 28 patients undergoing T-configured dual stent implantation to palliate malignant biliary hilar obstruction. The unilobar approach was first attempted in the procedure, which progressed to bilobar approach when it was found that the unilobar approach was not feasible. If the stent was again obstructed, clinical palliation was attempted using stent re-insertion or PTBD. Clinical factors associated with T-configured dual stenting were examined in the patients with stent re-obstruction, which was followed by a correlation between these clinical factors and stent obstruction.
RESULTS
Eleven of 13 patients were successfully treated by the unilobar approach. The two unsuccessful cases sustained angulation of the central large mesh stent. For the bilobar approach, 14 of 15 patients were successfully treated. For the one unsuccessful patient, the stent failed to pass through the central large mesh. Stent obstruction was revealed in 13 patients during the follow-up period. Balloon-assisted stent re-canalization was successfully performed in 5 patients. The analysis suggests that no definite correlation was found between stent obstruction and the clinical factors associated with dual stent placement. Conversely, bile containing sludge or debris was significantly correlated to early stent obstruction.
CONCLUSION
Technical adoption considering the bile duct anatomy and obstruction pattern is important for Tconfigured dual stent implantation. The prudent evaluation of bile juice characters and cholangiographic findings is required for the appropriate clinical application of the T-configured dual stenting.
MeSH Terms
Figure
-
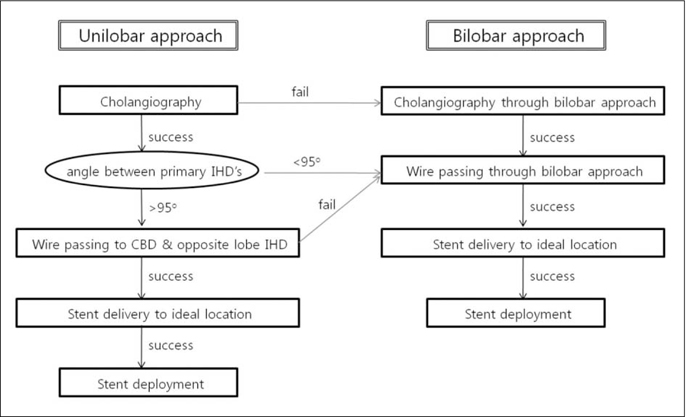
Fig. 1 Approaches for T-configured dual stent placement.

Fig. 2 Conventional technique of T-configured dual stent implantation (A) The large central mesh stent (*) is placed transversely, followed by insertion of an ordinary stent through large central mesh (white arrow). (B) The T-configured appearance of the deployed stents is demonstrated.

Fig. 3 Technical failure due to stent angulation at central large mesh portion (A) A 5F angled tip catheter passing from the right to the left hepatic duct reveals the angle between bilateral primary hepatic ducts is less than 90 degree. (B) T-configured dual stent implantation is achieved using conventional unilobar approaching technique, but angulating collapse of stent occurs subsequently at central large mesh portion.
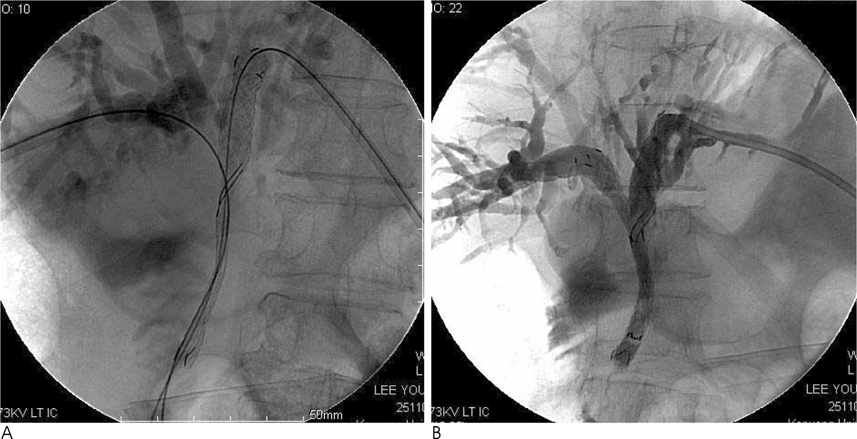
Fig. 4 T-configured dual stent implantation through bilobar approach in 70-year-old male patient with Klatskin tumor (A) Guidewires are passing to distal CBD through pre-existing PTBD in both hepatic lobes, and then a large central mesh stent is deployed vertically instead of transverse placement in conventional technique. Two guidewires reveal the angle formed by bilateral primary hepatic ducts is quite narrow. (B) An ordinary stent is implanted through the large central mesh, forming Y configuration.

Fig. 5 Ballooning and additional stent insertion to reopen occluded T-configured dual stents (A) A mesh of the ordinary vertical stent is dilated with a balloon. (B) A new large central mesh stent is inserted through the dilated mesh, making its large central mesh overlapped with that of the previously inserted large mesh stent. (C) A new vertical stent is inserted through the newly deployed large central mesh stent, to be placed in the previously inserted vertical stent.
Reference
-
1. Huibregtse K, Cheng J, Coene PP, Fockens P, Tytgat GN. Endoscopic placement of expandable metal stents for biliary strictures: a preliminary report on experience with 33 patients. Endoscopy. 1989; 21:280–282.2. Neuhaus H, Hagenmuller F, Classen M. Self-expanding biliary stents: preliminary clinical experience. Endoscopy. 1989; 21:225–228.3. Irving JD, Adam A, Dick R, Dondelinger RF, Lunderquist A, Roche A. Gianturco expandable metallic biliary stents: results of a European clinical trial. Radiology. 1989; 172:321–326.4. Lameris JS, Stoker J, Nijs HG, Zonderland HM, Terpstra OT, van Blankenstein M, et al. Malignant biliary obstruction: percutaneous use of self-expandible stents. Radiology. 1991; 179:703–707.5. Becker CD, Glattli A, Maibach R, Baer HU. Percutaneous palliation of malignant obstructive jaundice with the Wallstent endoprosthesis: follow-up and reintervention in patients with hilar and non-hilar obstruction. J Vasc Interv Radiol. 1993; 4:597–604.6. Tsai CC, Mo LR, Lin RC, Kuo JY, Chang KK, Yeh YH, et al. Selfexpandable metallic stents in the management of malignant biliary obstruction. J Formos Med Assoc. 1996; 95:298–302.7. Schima W, Prokesch R, Österreicher C, Thurnher S, Függer R, Schöfl R, et al. Biliary Wallstent endoprosthesis in malignant hilar obstruction: long-term results with regard to the type of obstruction. Clin Radiol. 1997; 52:213–219.8. Cheng JL, Bruno MJ, Bergman JJ, Rauws EA, Tytgat GN, Huibregtse K. Endoscopic palliation of patients with biliary obstruction caused by nonresectable hilar cholangiocarcinoma: efficacy of self-expandable metallic Wallstents. Gastrointest Endosc. 2002; 56:33–39.9. Chang WH, Kortan P, Haber GB. Outcome in patients with bifurcation tumors who undergo unilateral versus bilateral hepatic duct drainage. Gastrointest Endosc. 1998; 47:354–362.10. Lee BH, Choe DH, Lee JH, Kim KH, Chin SY. Metallic stents in malignant biliary obstruction: prospective long-term clinical results. AJR Am J Roentgenol. 1997; 168:741–745.11. Inal M, Akgul E, Aksungur E, Seydaoglu G. Percutaneous placement of biliary metallic stents in patients with malignant hilar obstruction: unilobar versus bilobar drainage. J Vasc Interv Radiol. 2003; 14:1409–1416.12. Lee MJ, Dawson SL, Mueller PR, Krebs TL, Saini S, Hahn PF. Palliation of malignant bile duct obstruction with metallic biliary endoprostheses: technique, results, and complications. J Vasc Interv Radiol. 1992; 3:665–671.13. Lee MJ, Dawson SL, Mueller PR, Saini S, Hahn PF, Goldberg MA, et al. Percutaneous management of hilar biliary malignancies with metallic endoprostheses: results, technical problems, and causes of failure. Radiographics. 1993; 13:1249–1263.14. Kubota Y, Nakatani S, Nakahashi Y, Takaoka M, Kin H, Inoue K. Bilateral internal biliary drainage of hilar cholangiocarcinoma with modified Gianturco Z stents inserted via a single percutaneous tract. J Vasc Interv Radiol. 1993; 4:605–610.15. Dumas R, Demuth N, Buckley M, Peten EP, Manos T, Demarquay JF, et al. Endoscopic bilateral metal stent placement for malignant hilar stenoses: identification of optimal technique. Gastrointest Endosc. 2000; 51:334–338.16. Neuhaus H, Gottlieb K, Classen M. The “stent through wire mesh technique” for complicated biliary strictures. Gastrointest Endosc. 1993; 39:553–556.17. Kim CW, Park AW, Won JW, Kim S, Lee JW, Lee SH. T-configured dual stent placement in malignant biliary hilar duct obstructions with a newly designed stent. J Vasc Interv Radiol. 2004; 15:713–717.18. Burke DR, McLean GK. Obstructions of the hepatic duct confluence: internal drainage of bilateral lesions with a single catheter. Radiology. 1989; 172:1035–1038.19. Uflacker R, Mourao GS, Piske RL, Lima S. Percutaneous transhepatic biliary drainage: alternative in left hepatic duct obstruction. Gastrointest Radiol. 1989; 14:137–142.20. Druy EM, Melville GE. Obstructed hepatic duct bifurcation: decompression via single percutaneous tract. AJR Am J Roentgenol. 1984; 143:73–76.21. LaBerge JM, Doherty M, Gordon RL, Ring EJ. Hilar malignancy: treatment with an expandable metallic transhepatic biliary stent. Radiology. 1990; 177:793–797.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Stent Placement in the Palliation of Malignant Biliary Obstruction
- Multiple metallic stents placement for malignant hilar biliary obstruction: Perspective of a radiologist
- Safety and Efficacy of Percutaneous Intraductal Radiofrequency Ablation Followed by Dual Stent Placement for Malignant Biliary Hilar Obstruction
- Endoscopic Bilateral Metal Stent Placement with a Y-Configured Dual Stent for Advanced Hilar Carcinoma
- Technical Tips and Issues of Biliary Stenting, Focusing on Malignant Hilar Obstruction
