Technical Tips and Issues of Biliary Stenting, Focusing on Malignant Hilar Obstruction
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. thlee9@schmc.ac.kr
- KMID: 2048931
- DOI: http://doi.org/10.5946/ce.2013.46.3.260
Abstract
- Although there is no survival advantage, inoperable hilar cholangiocarcinoma managed by palliative drainage may benefit from symptomatic improvement. In general, biliary drainage is divided into endoscopic or percutaneous approaches and surgical drainage. Plastic or metal stent is the most preferred device for palliative drainage in endoscopic approach. Considering cost-effectiveness, use of metallic stent is preferred than plastic stents in patients with more than 3 months of life expectancy with inoperable malignant biliary obstruction. In patients with unresectable malignant hilar obstruction, the endoscopic approach with biliary stent placement by experts has been considered as the treatment of choice. However, the endoscopic management of hilar obstruction is often more challenging and complex than distal malignant biliary obstructions. There is still a lack of clear consensus on the use of plastic versus metal stents and unilateral versus bilateral drainage since the decision should be made under many grounds such as the volume of liver drainage more than 50%, life expectancy, and expertise of the facility.
MeSH Terms
Figure
-
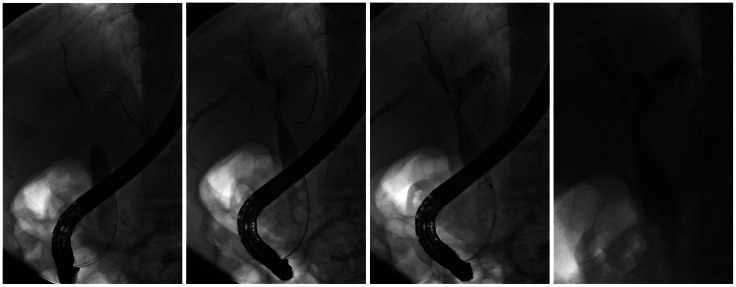
Fig. 1 Side-by-side deployment of metallic stents (Bonastent; Standard SciTech Inc.); sequential images of bilateral side-by-side stent placement in a patient with hilar cholangiocarcinoma (Bismuth type IIIA). The stricture was first negotiated with a guidewire inserted into the left hepatic duct, and the right hepatic duct was then accessed using the same method. Following the introduction of these two guidewires, the first stent (with a radiopaque X mark) was inserted in the left hepatic duct without removing the preloaded guidewire; the second stent was then deployed in the right hepatic duct using the same method.
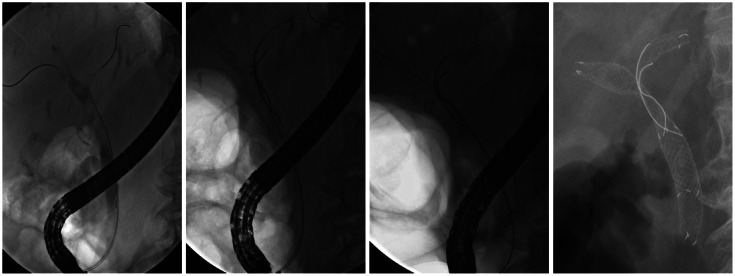
Fig. 2 Stent-in-stent deployment of metallic stents in Bismuth type IV (Bonastent; Standard SciTech Inc.); guidewires were initially introduced into both intrahepatic ducts bilaterally. The first stent with a radiopaque X mark was inserted into the left hepatic duct. After deployment of the first stent, the remaining guidewire was carefully withdrawn using an endoscopic retrograde cholangiopancreatography catheter, without pulling it back completely. The guidewire was then inserted into the right hepatic duct through the central portion of the first stent. Following deployment of the second stent, the bilateral metal stents were in a Y-configuration.
Cited by 6 articles
-
A Recent Update on Endoscopic Drainage of Advanced Malignant Hilar Obstruction
Tae Hoon Lee, Jong Ho Moon, Sang-Heum Park
Korean J Gastroenterol. 2021;78(2):94-104. doi: 10.4166/kjg.2021.111.A Recent Update on Endoscopic Drainage of Advanced Malignant Hilar Obstruction
Tae Hoon Lee, Jong Ho Moon, Sang-Heum Park
Korean J Gastroenterol. 2021;78(2):94-104. doi: 10.4166/kjg.2021.111.Clinical Outcomes of Bilateral Stent-in-Stent Placement Using Self-Expandable Metallic Stent for High-Grade Malignant Hilar Biliary Obstruction
Ja Yoon Heo, Hee Seung Lee, Jun Hyuk Son, Sang Hyub Lee, Seungmin Bang
Yonsei Med J. 2018;59(7):827-833. doi: 10.3349/ymj.2018.59.7.827.Editors' Choice of Noteworthy Clinical Endoscopy Publications in the First Decade
Gwang Ha Kim, Kwang An Kwon, Do Hyun Park, Jimin Han
Clin Endosc. 2021;54(5):633-640. doi: 10.5946/ce.2021.216.Highlights of the 48th Seminar of Korean Society of Gastrointestinal Endoscopy
Kwang An Kwon, Il Ju Choi, Eun Young Kim, Seok Ho Dong, Ki Baik Hahm
Clin Endosc. 2013;46(3):203-211. doi: 10.5946/ce.2013.46.3.203.Bilateral Metallic Stenting in Malignant Hilar Obstruction
Tae Hoon Lee, Jong Ho Moon, Sang-Heum Park
Clin Endosc. 2014;47(5):440-446. doi: 10.5946/ce.2014.47.5.440.
Reference
-
1. Kim JH. Endoscopic stent placement in the palliation of malignant biliary obstruction. Clin Endosc. 2011; 44:76–86. PMID: 22741117.
Article2. Wagner HJ, Knyrim K, Vakil N, Klose KJ. Plastic endoprostheses versus metal stents in the palliative treatment of malignant hilar biliary obstruction. A prospective and randomized trial. Endoscopy. 1993; 25:213–218. PMID: 7686100.
Article3. Raijman I. Biliary and pancreatic stents. Gastrointest Endosc Clin N Am. 2003; 13:561–592. PMID: 14986787.
Article4. Maillot N, Aucher P, Robert S, et al. Polyethylene stent blockage: a porcine model. Gastrointest Endosc. 2000; 51:12–18. PMID: 10625788.
Article5. Speer AG, Cotton PB, MacRae KD. Endoscopic management of malignant biliary obstruction: stents of 10 French gauge are preferable to stents of 8 French gauge. Gastrointest Endosc. 1988; 34:412–417. PMID: 2460394.
Article6. Pedersen FM. Endoscopic management of malignant biliary obstruction. Is stent size of 10 French gauge better than 7 French gauge? Scand J Gastroenterol. 1993; 28:185–189. PMID: 8441913.
Article7. Kadakia SC, Starnes E. Comparison of 10 French gauge stent with 11.5 French gauge stent in patients with biliary tract diseases. Gastrointest Endosc. 1992; 38:454–459. PMID: 1511821.
Article8. van Berkel AM, Boland C, Redekop WK, et al. A prospective randomized trial of Teflon versus polyethylene stents for distal malignant biliary obstruction. Endoscopy. 1998; 30:681–686. PMID: 9865556.
Article9. England RE, Martin DF, Morris J, et al. A prospective randomised multicentre trial comparing 10 Fr Teflon Tannenbaum stents with 10 Fr polyethylene Cotton-Leung stents in patients with malignant common duct strictures. Gut. 2000; 46:395–400. PMID: 10673303.
Article10. Terruzzi V, Comin U, De Grazia F, et al. Prospective randomized trial comparing Tannenbaum Teflon and standard polyethylene stents in distal malignant biliary stenosis. Gastrointest Endosc. 2000; 51:23–27. PMID: 10625790.
Article11. Davids PH, Groen AK, Rauws EA, Tytgat GN, Huibregtse K. Randomised trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet. 1992; 340:1488–1492. PMID: 1281903.
Article12. Kaassis M, Boyer J, Dumas R, et al. Plastic or metal stents for malignant stricture of the common bile duct? Results of a randomized prospective study. Gastrointest Endosc. 2003; 57:178–182. PMID: 12556780.
Article13. Schmassmann A, von Gunten E, Knuchel J, Scheurer U, Fehr HF, Halter F. Wallstents versus plastic stents in malignant biliary obstruction: effects of stent patency of the first and second stent on patient compliance and survival. Am J Gastroenterol. 1996; 91:654–659. PMID: 8677925.14. Pedersen FM, Lassen AT, Schaffalitzky de Muckadell OB. Randomized trial of stent placed above and across the sphincter of Oddi in malignant bile duct obstruction. Gastrointest Endosc. 1998; 48:574–579. PMID: 9852446.
Article15. Park do H, Lee SS, Moon JH, et al. Newly designed stent for endoscopic bilateral stent-in-stent placement of metallic stents in patients with malignant hilar biliary strictures: multicenter prospective feasibility study (with videos). Gastrointest Endosc. 2009; 69:1357–1360. PMID: 19481654.
Article16. Dowsett JF, Vaira D, Hatfield AR, et al. Endoscopic biliary therapy using the combined percutaneous and endoscopic technique. Gastroenterology. 1989; 96:1180–1186. PMID: 2925062.
Article17. Polydorou AA, Cairns SR, Dowsett JF, et al. Palliation of proximal malignant biliary obstruction by endoscopic endoprosthesis insertion. Gut. 1991; 32:685–689. PMID: 1711994.
Article18. Chahal P, Baron TH. Expandable metal stents for endoscopic bilateral stent-within-stent placement for malignant hilar biliary obstruction. Gastrointest Endosc. 2010; 71:195–199. PMID: 19945101.
Article19. Kawamoto H, Tsutsumi K, Fujii M, et al. Endoscopic 3-branched partial stent-in-stent deployment of metallic stents in high-grade malignant hilar biliary stricture (with videos). Gastrointest Endosc. 2007; 66:1030–1037. PMID: 17963891.20. Jarnagin WR, Fong Y, DeMatteo RP, et al. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma. Ann Surg. 2001; 234:507–517. PMID: 11573044.
Article21. Perdue DG, Freeman ML, DiSario JA, et al. Plastic versus self-expanding metallic stents for malignant hilar biliary obstruction: a prospective multicenter observational cohort study. J Clin Gastroenterol. 2008; 42:1040–1046. PMID: 18719507.22. Raju RP, Jaganmohan SR, Ross WA, et al. Optimum palliation of inoperable hilar cholangiocarcinoma: comparative assessment of the efficacy of plastic and self-expanding metal stents. Dig Dis Sci. 2011; 56:1557–1564. PMID: 21222156.
Article23. Stern N, Sturgess R. Endoscopic therapy in the management of malignant biliary obstruction. Eur J Surg Oncol. 2008; 34:313–317. PMID: 18276101.
Article24. Rerknimitr R, Angsuwatcharakon P, Ratanachu-Ek T, et al. Asia-Pacific consensus recommendations for endoscopic and interventional management of hilar cholangiocarcinoma. J Gastroenterol Hepatol. 2013; 28:593–607. PMID: 23350673.
Article25. Polydorou AA, Chisholm EM, Romanos AA, et al. A comparison of right versus left hepatic duct endoprosthesis insertion in malignant hilar biliary obstruction. Endoscopy. 1989; 21:266–271. PMID: 2482169.
Article26. De Palma GD, Galloro G, Siciliano S, Iovino P, Catanzano C. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc. 2001; 53:547–553. PMID: 11323577.
Article27. De Palma GD, Pezzullo A, Rega M, et al. Unilateral placement of metallic stents for malignant hilar obstruction: a prospective study. Gastrointest Endosc. 2003; 58:50–53. PMID: 12838220.
Article28. Sherman S. Endoscopic drainage of malignant hilar obstruction: is one biliary stent enough or should we work to place two? Gastrointest Endosc. 2001; 53:681–684. PMID: 11323609.
Article29. Iwano H, Ryozawa S, Ishigaki N, et al. Unilateral versus bilateral drainage using self-expandable metallic stent for unresectable hilar biliary obstruction. Dig Endosc. 2011; 23:43–48.
Article30. Nomura T, Shirai Y, Hatakeyama K. Cholangitis after endoscopic biliary drainage for hilar lesions. Hepatogastroenterology. 1997; 44:1267–1270. PMID: 9356838.31. Freeman ML, Overby C. Selective MRCP and CT-targeted drainage of malignant hilar biliary obstruction with self-expanding metallic stents. Gastrointest Endosc. 2003; 58:41–49. PMID: 12838219.
Article32. Hintze RE, Abou-Rebyeh H, Adler A, Veltzke-Schlieker W, Felix R, Wiedenmann B. Magnetic resonance cholangiopancreatography-guided unilateral endoscopic stent placement for Klatskin tumors. Gastrointest Endosc. 2001; 53:40–46. PMID: 11154487.
Article33. Khan SA, Davidson BR, Goldin R, et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: consensus document. Gut. 2002; 51(Suppl 6):VI1–VI9. PMID: 12376491.
Article34. Chang WH, Kortan P, Haber GB. Outcome in patients with bifurcation tumors who undergo unilateral versus bilateral hepatic duct drainage. Gastrointest Endosc. 1998; 47:354–362. PMID: 9609426.
Article35. Naitoh I, Ohara H, Nakazawa T, et al. Unilateral versus bilateral endoscopic metal stenting for malignant hilar biliary obstruction. J Gastroenterol Hepatol. 2009; 24:552–557. PMID: 19220678.
Article36. Saleem A, Baron TH, Gostout CJ. Large-diameter therapeutic channel duodenoscope to facilitate simultaneous deployment of side-by-side self-expandable metal stents in hilar cholangiocarcinoma. Gastrointest Endosc. 2010; 72:628–631. PMID: 20579649.
Article37. Kwon AH, Uetsuji S, Ogura T, Kamiyama Y. Spiral computed tomography scanning after intravenous infusion cholangiography for biliary duct anomalies. Am J Surg. 1997; 174:396–401. PMID: 9337161.
Article38. Cheng JL, Bruno MJ, Bergman JJ, Rauws EA, Tytgat GN, Huibregtse K. Endoscopic palliation of patients with biliary obstruction caused by nonresectable hilar cholangiocarcinoma: efficacy of self-expandable metallic Wallstents. Gastrointest Endosc. 2002; 56:33–39. PMID: 12085032.
Article39. Dumas R, Demuth N, Buckley M, et al. Endoscopic bilateral metal stent placement for malignant hilar stenoses: identification of optimal technique. Gastrointest Endosc. 2000; 51:334–338. PMID: 10699784.
Article40. Chennat J, Waxman I. Initial performance profile of a new 6F self-expanding metal stent for palliation of malignant hilar biliary obstruction. Gastrointest Endosc. 2010; 72:632–636. PMID: 20579991.
Article41. Lee JH, Kang DH, Kim JY, et al. Endoscopic bilateral metal stent placement for advanced hilar cholangiocarcinoma: a pilot study of a newly designed Y stent. Gastrointest Endosc. 2007; 66:364–369. PMID: 17643714.42. Kim JY, Kang DH, Kim HW, et al. Usefulness of slimmer and open-cell-design stents for endoscopic bilateral stenting and endoscopic revision in patients with hilar cholangiocarcinoma (with video). Gastrointest Endosc. 2009; 70:1109–1115. PMID: 19647244.
Article43. Hwang JC, Kim JH, Lim SG, Kim SS, Yoo BM, Cho SW. Y-shaped endoscopic bilateral metal stent placement for malignant hilar biliary obstruction: prospective long-term study. Scand J Gastroenterol. 2011; 46:326–332. PMID: 21082874.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Metallic Stenting in Malignant Hilar Obstruction
- Endoscopic Stenting for Malignant Biliary Obstruction: Results of a Nationwide Experience
- Endoscopic Ultrasound-Guided Biliary Drainage for Unresectable Hilar Malignant Biliary Obstruction
- Endoscopic Ultrasound-Guided Hepaticogastrostomy: Technical Review and Tips to Prevent Adverse Events
- Percutaneous Transhepatic Recanalization of Malignant Hilar Obstruction: A Possible Rescue for Early Failure of Endoscopic Y-Stenting
