Percutaneous Transhepatic Recanalization of Malignant Hilar Obstruction: A Possible Rescue for Early Failure of Endoscopic Y-Stenting
- Affiliations
-
- 1Department of Radiology, Pusan National University School of Medicine, Pusan National University Hospital, Busan, Korea. radkim@nate.com
- 2Department of Radiology, Pusan National University School of Medicine, Yangsan Pusan National University Hospital, Yangsan, Korea.
- 3Department of Internal Medicine, Pusan National University School of Medicine, Pusan National University Hospital, Busan, Korea.
- 4Department of Internal Medicine, Pusan National University School of Medicine, Yangsan Pusan National University Hospital, Yangsan, Korea.
- KMID: 2002860
- DOI: http://doi.org/10.3348/jksr.2013.69.5.385
Abstract
- PURPOSE
Endoscopic biliary stenting is well known as an optimal method of management of malignant hilar obstruction, but sometimes the result is not satisfactory, with early stent failure. Percutaneous transhepatic biliary drainage (PTBD) has a distinct advantage over endoscopic retrograde cholangiopancreatoscopy in that with ultrasound guidance one or more appropriate segments for drainage can be chosen. We evaluated the effectiveness of percutaneous transhepatic stenting as a rescue of early failure of endoscopic stenting.
MATERIALS AND METHODS
Ten patients (4 men, 6 women; age range, 52-78 years; mean age, 69 years) with inoperable biliary obstruction (2 patients with gall bladder cancer and hilar invasion, and 8 patients with Klatskin tumor) and with early endoscopic stent failure were included in our study. All of the patients underwent PTBD and percutaneous transhepatic biliary stenting. Metallic stents were placed in all patients for internal drainage.
RESULTS
Percutaneous rescue stenting was successful in all the patients technically and clinically. Mean time for the development of biliary obstruction was 13.5 days after endoscopic stenting. The mean patency of the rescue stenting was 122 days. The mean survival time for percutaneous transhepatic rescue stenting was 226.3 days.
CONCLUSION
In early failure of endoscopic biliary stenting, percutaneous transhepatic recanalization can be a possible solution.
MeSH Terms
Figure
-
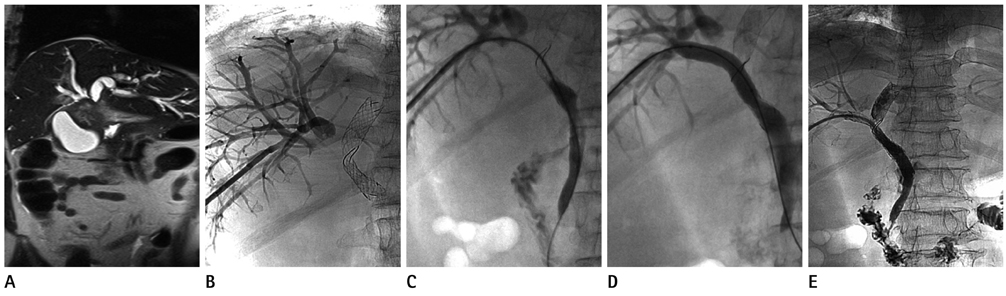
Fig. 1 Patient 1, 68-year-old female, gall bladder (GB) cancer with hilar invasion, Bismuth IIIA obstruction. A. Coronal T2-weighted MR image shows GB mass with hilar invasion. B. Cause of endoscpopic stent failure was second stent (endoscopic Y-stent) insertion failure. Cholangiogram shows obstruction of right hepatic duct. C. The stricture was negotiated with the use of guide wire and catheter technique. Cholangiogram shows passage of the guide wire. D. After passage of the guidewire, a balloon catheter was used for dilatation of stricture. E. Rescue stenting was performed by Niti-D 10/70 mm. Final cholangiogram shows good communication of the whole biliary system.

Fig. 2 Patient 6, 63-year-old female, Klatskin tumor, Bismuth IV. A. Coronal T2-weighted MR image shows hilar mass with prominent bile duct dilatation. B. Cholangiogram shows obstruction of right hepatic duct and malposition of endoscopic Y-stent in B4 and left hepatic duct. C. Rescue stenting was performed by Luminexx 10/80 mm.
Reference
-
1. Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis. An unusual tumor with distinctive clinical and pathological features. Am J Med. 1965; 38:241–256.2. Nakeeb A, Pitt HA, Sohn TA, Coleman J, Abrams RA, Piantadosi S, et al. Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. Ann Surg. 1996; 224:463–473. discussion 473-475.3. Ogura Y, Mizumoto R, Tabata M, Matsuda S, Kusuda T. Surgical treatment of carcinoma of the hepatic duct confluence: analysis of 55 resected carcinomas. World J Surg. 1993; 17:85–92. discussion 92-93.4. Kim CW, Park AW, Won JW, Kim S, Lee JW, Lee SH. T-configured dual stent placement in malignant biliary hilar duct obstructions with a newly designed stent. J Vasc Interv Radiol. 2004; 15:713–717.5. Lee JH, Kang DH, Kim JY, Lee SM, Kim do H, Park CW, et al. Endoscopic bilateral metal stent placement for advanced hilar cholangiocarcinoma: a pilot study of a newly designed Y stent. Gastrointest Endosc. 2007; 66:364–369.6. Hwang JC, Kim JH, Lim SG, Kim SS, Yoo BM, Cho SW. Y-shaped endoscopic bilateral metal stent placement for malignant hilar biliary obstruction: prospective long-term study. Scand J Gastroenterol. 2011; 46:326–332.7. Kawamoto H, Tsutsumi K, Harada R, Fujii M, Kato H, Hirao K, et al. Endoscopic deployment of multiple JOSTENT SelfX is effective and safe in treatment of malignant hilar biliary strictures. Clin Gastroenterol Hepatol. 2008; 6:401–408.8. Kim JY, Kang DH, Kim HW, Choi CW, Kim ID, Hwang JH, et al. Usefulness of slimmer and open-cell-design stents for endoscopic bilateral stenting and endoscopic revision in patients with hilar cholangiocarcinoma (with video). Gastrointest Endosc. 2009; 70:1109–1115.9. Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991; 37:383–393.10. Ferrucci JT Jr, Mueller PR, Harbin WP. Percutaneous transhepatic biliary drainage: technique, results, and applications. Radiology. 1980; 135:1–13.11. Ridtitid W, Rerknimitr R, Janchai A, Kongkam P, Treeprasertsuk S, Kullavanijaya P. Outcome of second interventions for occluded metallic stents in patients with malignant biliary obstruction. Surg Endosc. 2010; 24:2216–2220.12. Paik WH, Park YS, Hwang JH, Lee SH, Yoon CJ, Kang SG, et al. Palliative treatment with self-expandable metallic stents in patients with advanced type III or IV hilar cholangiocarcinoma: a percutaneous versus endoscopic approach. Gastrointest Endosc. 2009; 69:55–62.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Ultrasound-Guided Biliary Drainage for Unresectable Hilar Malignant Biliary Obstruction
- Bilateral Metallic Stenting in Malignant Hilar Obstruction
- Percutaneous transhepatic access to allow per-oral enteric stent insertion for malignant duodenal obstruction following failed endoscopic attempt
- Technical Tips and Issues of Biliary Stenting, Focusing on Malignant Hilar Obstruction
- Endoscopic Stenting for Malignant Biliary Obstruction: Results of a Nationwide Experience
