Two Breast Metastases from Thyroid Carcinoma Presented 6 Years Later after Total Thyroidectomy: A Case Report
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. lionmain@catholic.ac.kr
- 2Department of Radiology, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Bucheon, Korea.
- 3Department of Hospital Pathology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2208786
- DOI: http://doi.org/10.3348/jksr.2016.74.4.267
Abstract
- Thyroid carcinoma is usually indolent with good prognosis, as compared to other malignancy. Distant metastases from thyroid cancer are rare and usually manifest as multiple lesions especially in lungs, bones and lymph nodes, in advanced stages of the disease. Metastasis to the breast from thyroid carcinoma is extremely rare, with about 16 cases reported in the English literature. Herein, we reported a case of metastatic poorly differentiated thyroid carcinoma, which presented as 2 breast masses in a 72-year-old woman, 6 years after total thyroidectomy for papillary thyroid carcinoma. Although the computed tomography (CT) and ultrasonography (USG) image findings are nonspecific oval mass with circumscribed or partially indistinct margin, metastases from thyroid cancer should be included in the differential diagnosis when recurrence of thyroid carcinoma is suspected. Also, fusion images of CT and USG are helpful to the radiologists in localizing the targeted lesion and conducting accurate USG-guided biopsy.
MeSH Terms
Figure
-
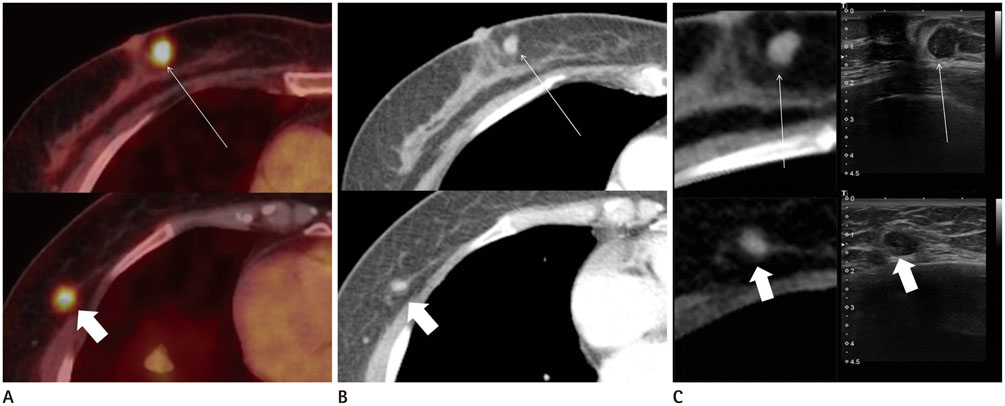
Fig. 1 Imaging findings of metastatic tumors in the right breast from thyroid carcinoma in a 72-year-old woman, 6 years after initial thyroidectomy. A-C. Periareolar lesion in the 3 o'clock direction (long thin white arrows; upper column) and another peripheral lesion in the 8 o'clock direction (short thick white arrows; lower column) of the right breast are shown in the positron emission tomography/computed tomography (PET/CT), chest CT, ultrasonography (USG), and CT navigated USG fusion images. 18F-fluorodeoxyglucose (FDG) uptake in 2 nodular lesions on axial image of PET/CT (A) is noted in the inner portion and outer lower portion of the right breast. The lesions are soft tissue attenuated and homogenously enhanced after contrast injection on axial image of chest CT scan (B). On CT navigated USG fusion images (C), the periareolar lesion is oval, circumscribed, non-parallel oriented mass with hypo- to isoechogenicity, surrounded by premammary fat. The other lesion is visualized as oval, partially indistinct marginated and hypoechoic mass with parallel orientation. CT navigated USG fusion image reaffirms that prior FDG-avid nodules are matched to the hypoechoic masses on sonogram, surrounded by fat.
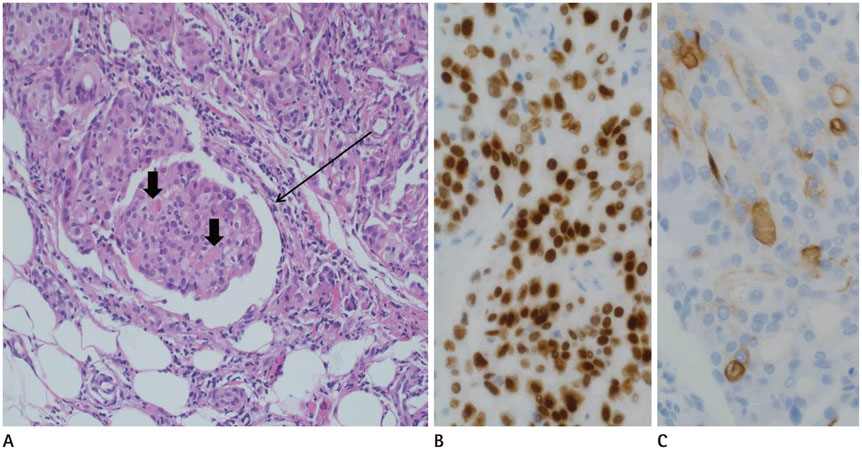
Fig. 2 Pathologic findings of metastatic tumors in the right breast from thyroid carcinoma in a 72-year-old woman, 6 years after initial thyroidectomy. A. Microscopic photomicrograph illustrates that small nests of tumor cells are predominantly solid and focally contain eosinophilic colloidal materials (short thick black arrows). The neoplastic cell nests show increased mitosis and locate within cells of a mammary duct and interstitium (long thin black arrow) (original magnification, × 200; H&E stain). B, C. Immunohistochemical staining shows the tumor cells are positive for TTF1 (B) and thyroglobulin (C), which appear brown suggestive of thyroid tissue origin (original magnification, × 400). Scanty expression of thyroglobulin and increased Ki-67 labeling index confirms thyroid carcinoma with poor differentiation. H&E = hematoxylin and eosin, TTF1 = thyroid transcription factor-1
Reference
-
1. Loureiro MM, Leite VH, Boavida JM, Raposo JF, Henriques MM, Limbert ES, et al. An unusual case of papillary carcinoma of the thyroid with cutaneous and breast metastases only. Eur J Endocrinol. 1997; 137:267–269.2. Song HJ, Xue YL, Xu YH, Qiu ZL, Luo QY. Rare metastases of differentiated thyroid carcinoma: pictorial review. Endocr Relat Cancer. 2011; 18:R165–R174.3. Akçay MN. Metastatic disease in the breast. Breast. 2002; 11:526–528.4. Ordóñez NG, Katz RL, Luna MA, Samaan NA. Medullary thyroid carcinoma metastatic to breast diagnosed by fine-needle aspiration biopsy. Diagn Cytopathol. 1988; 4:254–257.5. Cristallini EG, Ascani S, Nati S, Liberati F, Farabi R. Breast metastasis of thyroid follicular carcinoma. Acta Oncol. 1994; 33:71–73.6. Chisholm RC, Chung EB, Tuckson W, Khan T, White JE. Follicular carcinoma of the thyroid with metastasis to the breast. J Natl Med Assoc. 1980; 72:1101–1104.7. Angeles-Angeles A, Chable-Montero F, Martinez-Benitez B, Albores-Saavedra J. Unusual metastases of papillary thyroid carcinoma: report of 2 cases. Ann Diagn Pathol. 2009; 13:189–196.8. Al-Abed Y, Gray E, Wolfe K, Watters GW, Philpott JM. Metastatic Hurthle Cell Carcinoma of the thyroid presenting as a breast lump: a case report. Int Semin Surg Oncol. 2008; 5:14.9. Mandanas S, Margaritidou E, Christoforidou V, Karoglou E, Geranou C, Chrisoulidou A, et al. Breast metastasis from medullary thyroid carcinoma in a male patient: case report and review of the literature. Rare Tumors. 2015; 7:5765.10. Marcy PY, Thariat J, Peyrottes I, Dassonville O. Bilateral breast involvement in medullary thyroid carcinoma. Thyroid. 2009; 19:197–199.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasonographic Features and the Diagnostic Role of Core Needle Biopsy at Metastatic Breast Cancer in the Thyroid gland: A Case Report
- Bilateral axillo-breast approach robotic total thyroidectomy without isthmectomy: a case report
- A Case of Scalp Metastasis from Follicular Thyroid Carcinoma
- Metastatic Medullary Carcinoma of Thyroid to Breast; A Case Initially Diagnosed as Primary Invasive Lobular Carcinoma: A Case Report
- Subcutaneous Soft Tissue Implantation of Papillary Thyroid Carcinoma after Endoscopic Thyroidectomy
