J Menopausal Med.
2015 Apr;21(1):56-59. 10.6118/jmm.2015.21.1.56.
Postmenopausal Meigs' Syndrome in Elevated CA-125: A Case Report
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Dong-A University, College of Medicine, Busan, Korea. jwbae@dau.ac.kr
- KMID: 2201023
- DOI: http://doi.org/10.6118/jmm.2015.21.1.56
Abstract
- Meigs' syndrome is a benign ovarian tumor associated with ascites and pleural effusion. Elevated cancer antigen 125 (CA-125) in Meigs' syndrome is an unusual clinical condition reported in few cases. We report here on a 61-year-old woman who presented with dyspnea; in imaging assessment, a heterogeneous pelvic mass measuring 12 x 11 cm with ascitic fluid was reported. Pleural effusion was detected on Chest X-ray. Aspiration of pleural fluid showed no evidence of malignancy. CA-125 level was 347 IU/mL. The patient underwent laparotomy during which a mass measuring 12 x 11 cm was detected in her left adnexa. Histology showed ovarian thecoma. The mass was resected, and, after that, the symptoms disappeared and CA-125 level reached 19 IU/mL. The patient had experienced no problem after 12 months of follow up. Although postmenopausal women with ovarian tumor, ascites, pleural effusion, and elevation of CA-125 levels probably have malignant ovarian tumors, Meigs' syndrome must be considered in the differential diagnosis.
Keyword
MeSH Terms
Figure
-

Fig. 1 A chest X-ray revealed the presence of a massive right sided pleural effusion.

Fig. 2 Abdominopelvic computed tomography scan revealed a solid heterogeneous mass in pelvic midline with ascites.
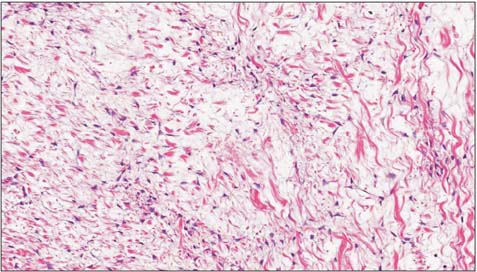
Fig. 3 The tumor cells have bland, oval to spindle shaped nuclei and abundant, pale vacuolated cytoplasm. Individual tumor cells are invested by thin reticulin fibers (H&E × 400).
Reference
-
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005; 55:74–108.2. Meigs JV. Fibroma of the ovary with ascites and hydrothorax; Meig's syndrome. Am J Obstet Gynecol. 1954; 67:962–985.3. Benjapibal M, Sangkarat S, Laiwejpithaya S, Viriyapak B, Chaopotong P, Jaishuen A. Meigs' Syndrome with Elevated Serum CA125: Case Report and Review of the Literature. Case Rep Oncol. 2009; 2:61–66.4. Turan YH, Demirel LC, Ortaç F. Elevated CA 125 in Meigs syndrome. Int J Gynaecol Obstet. 1993; 43:64–65.5. Abramov Y, Anteby SO, Fasouliotis SJ, Barak V. The role of inflammatory cytokines in Meigs' syndrome. Obstet Gynecol. 2002; 99:917–919.6. Agranoff D, May D, Jameson C, Knowles GK. Pleural effusion and a pelvic mass. Postgrad Med J. 1998; 74:265–267.7. Mui MP, Tam KF, Tam FK, Ngan HY. Coexistence of struma ovarii with marked ascites and elevated CA-125 levels: case report and literature review. Arch Gynecol Obstet. 2009; 279:753–757.8. Bast RC Jr, Feeney M, Lazarus H, Nadler LM, Colvin RB, Knapp RC. Reactivity of a monoclonal antibody with human ovarian carcinoma. J Clin Invest. 1981; 68:1331–1337.9. Kabawat SE, Bast RC Jr, Bhan AK, Welch WR, Knapp RC, Colvin RB. Tissue distribution of a coelomic-epithelium-related antigen recognized by the monoclonal antibody OC125. Int J Gynecol Pathol. 1983; 2:275–285.10. Jacobs I, Bast RC Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989; 4:1–12.11. Kudlacek S, Schieder K, Kölbl H, Neunteufel W, Nowotny C, Breitenecker G, et al. Use of CA 125 monoclonal antibody to monitor patients with ovarian cancer. Gynecol Oncol. 1989; 35:323–329.12. O'Connell GJ, Ryan E, Murphy KJ, Prefontaine M. Predictive value of CA 125 for ovarian carcinoma in patients presenting with pelvic masses. Obstet Gynecol. 1987; 70:930–932.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 1 case of Meigs' syndrome with markedly elevated serum CA 125 level
- A case of Meigs' syndrome with elevated serum CA 125 level
- A Case of Meigs` Syndrome with Elevated Serum CA 125 Level
- Meigs' Syndrome with Elevated Cancer Antigen 125
- Struma Ovarii Asssociated with Pseudo-Meigs' Syndrome and Elevated Serum CA 125
