J Korean Soc Endocrinol.
2005 Jun;20(3):283-288. 10.3803/jkes.2005.20.3.283.
A Case of Pheochromocytoma Presented with Cardiogenic Shock
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2200570
- DOI: http://doi.org/10.3803/jkes.2005.20.3.283
Abstract
- A pheochromocytoma is a catecholamine secreting tumor, which is often overlooked when cardiovascular complications, such as acute heart failure, myocardial infarction, angina pectoris, arrhythmias, and dilated cardiomyopathy, presented as the initial clinical manifestations. Failure to identify a pheochromocytoma in these situations may be fatal. We report the case of 32-year-old female, who presented with cardiogenic shock. Echocardiography revealed severe global hypokinesia of the dilated left ventricle, with the exception of the apex. Computed tomography of the aorta showed a well-enhanced left adrenal mass, 3.5cm in diameter. A 24 hour urine collection study for catecholamines and a 131I-metaiodobenzylguanidine(MIBG) scan were suggestive of the diagnosis of a single adrenal pheochromocytoma. The patient stabilized after shock management, and recovered with intensive medical treatment. Follow-up echocardiography revealed normalized cardiac function and chamber dimensions. Thereafter, the adrenal mass was successfully removed using laparaoscopic surgery, without complications
MeSH Terms
Figure
-
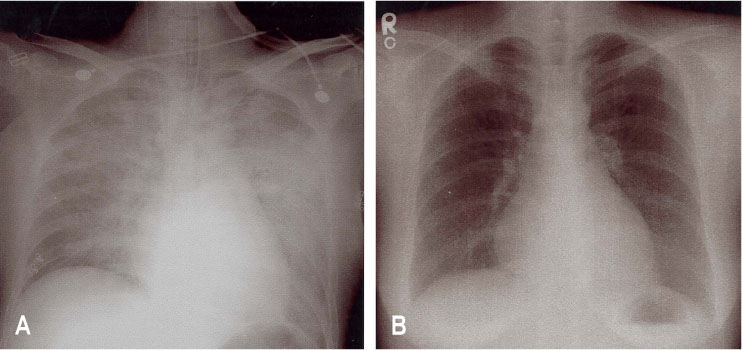
Fig. 1 A. At the emergency room, chest X-ray shows acute bilateral pulmonary edema. B. After medical treatment, chest X-ray shows the disappearance of pulmonary edema.

Fig. 2 A. The initial echocardiography revealed the dilatation and hypokinesia of left ventricle. B. After recovery, follow-up echocardiography revealed the normal chamber and function of left ventricle
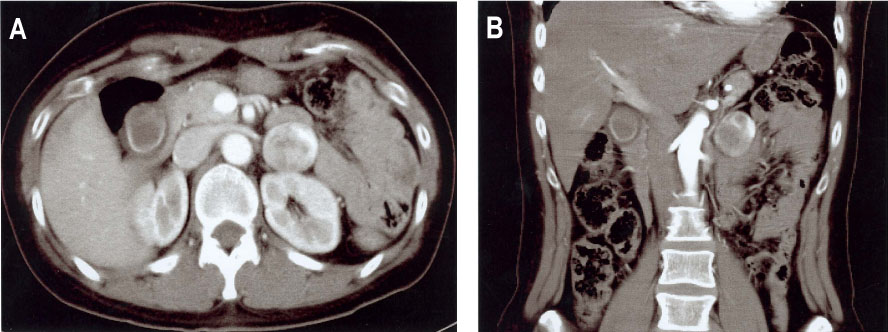
Fig. 3 Computed tomography revealed a well-circumscribed round mass in the left adrenal gland. (A: cross section, B: coronal section)
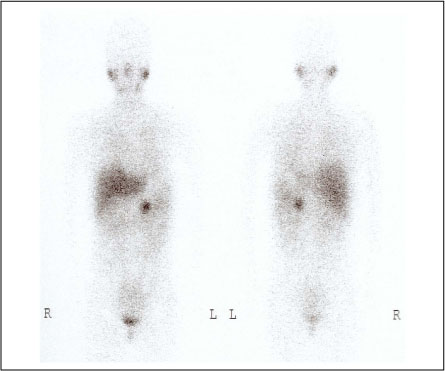
Fig. 4 I131 MIBG scan shows the single hot uptake at the left adrenal gland.
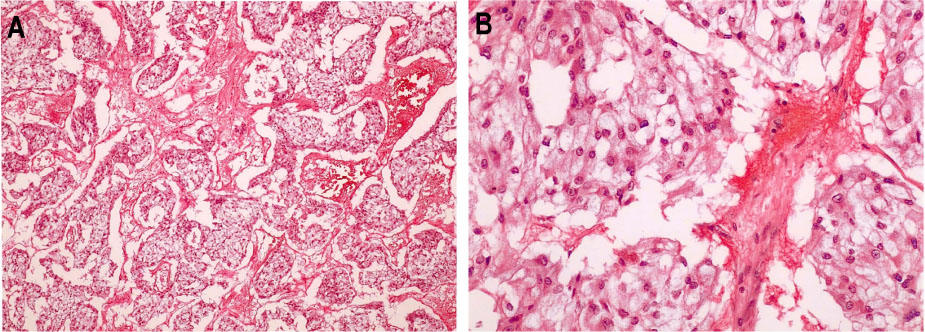
Fig. 5 Tumor cells have eosinophillic cytoplasm and polygonal shape, and are surrounded by mesenchyma of vasculature (H-E stain, A: ×200, B: ×400).
Reference
-
1. Sardesai SH, Mourant AJ, Sivathandon Y, Farrow R, Gibbons DO. Pheochromocytoma and catecholamine induced cardiomyopathy presenting as heart failure. Br Heart J. 1990. 63:234–237.2. Velasquez G, D'Souza VJ, Jackshaw BT, Glass TA, Formanek AG. Pheochromocytoma and cardiomyopathy. Br J Radiol. 1984. 57:89–92.3. Delaney J, Paritzky Z. Necrosis of a pheochromocytoma with shock. New Engl J Med. 1969. 280:1394–1395.4. Raman GV. Pheochromocytoma presenting with cardiogenic shock and acute renal failure. J Human Hypertension. 1987. 1:237–238.5. Scott I, Parkes R, Cameron DP. Phaeochromocytoma and cardiomyopathy. Med J Aust. 1988. 148:94–96.6. Ferguson KL. Imipramine-provoked paradoxical pheochormocytoma crisis case of cardiogenic shock. AmJ Emerg Med. 1994. 12:190–192.7. Takagi S, Miyazaki S, Fujii T, Daikoku S, Sutani Y, Morii I, Yasuda S, Goto Y, Nonogi H. Dexamethasone-induced cardiogenic shock rescued by percutaneous cardiopulmonary support in a patient with pheochromocytoma. Jpn Circ J. 2000. 64:785–788.9. Kaye J, Edin S, Thompson I, Leedma PJ. Pheochromocytoma presenting as life-threatening pulmonary edema. Endocrine. 2001. 15:203–204.10. Imperadore F, Azzolini M, Piscioli F, Pusiol T, Capitanio A, Vergara G. A rare cause of cardiogenic shock: catecholamine cardiomyopathy of pheochromocytoma. Ital Heart J. 2002. 3:375–378.11. Mohamed HA, Aldakar MO, Habib N. Cardiogenic shock due to acute hemorrhagic necrosis of a pheocromocytoma: a case report and review of the liter ature. Can J Cardiol. 2003. 19:573–576.12. Hildebrand TS, Bockholdt B, Jurgensen J. Neoplastic shock. Heart. 2004. 90:19.13. Imperato-Mcginley J, Gautier T, Ehlers K, Zullo MA, Goldstein DS, Vauhan ED. Reversibility of catecholamine induced cardiomyopathy in a child with a pheochromocytoma. N Eng J Med. 1987. 316:793–797.14. Attar MN, Moulik PK, Salem GD, Rose EL, Khaleeli AA. Pheochromocytoma presenting as dilated cardiomyopathy. Int J Clin Pract. 2003. 57:547–548.16. Rona G. Catecholamine cardiotoxicity. J Mol Cell Cardiol. 1985. 17:291–306.17. Kothari SN, Kisken WA. Dexamethasone-induced congestive heart failure in a patient with dilated cardiomyopathy caused by occult pheochromocytoma. Surgery. 1998. 123:102–105.18. Landsberg L, Young JB. Kasper DL, Braunwald E, Fauci AS, Hauser S, Longo DL, Jameson JL, editors. Pheochromocytoma. Harrison's textbook of medicine. 2005. 16th ed. New York: McGraw-Hill;2148–2152.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pheochromocytoma Presented with Cardiogenic Shock and Followed by Spontaneous Remission
- A Case of Pheochromocytoma Presented with Severe Left Ventricular Dysfunction Combined with Cardiogenic Shock after Caesearian Section Delivery Responding to Treatment of Extracorporeal Membrane Oxygenation
- Catastrophic catecholamine-induced cardiomyopathy rescued by extracorporeal membrane oxygenation in recurrent malignant pheochromocytoma
- Pheochromocytoma-induced cardiogenic shock successfully treated by extracorporeal circulation
- A Case of Pheochromocytoma Presented with Life: Threatening Cardiogenic Shock
