Differential diagnosis of common shoulder pain
- Affiliations
-
- 1Department of Rehabilitation Medicine, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea. hjrhee1@dumc.or.kr
- KMID: 2194915
- DOI: http://doi.org/10.5124/jkma.2014.57.8.653
Abstract
- Shoulder pain is a common problem in outpatient medical practice. Shoulder pain usually causes disability in activities of daily living, and therefore its proper diagnosis and management are essential. The prevalence of shoulder pain in Korea has been gradually increasing, and the differential diagnosis of shoulder pain has become more important. In Korea, the most common causes of shoulder pain are rotator cuff disease, including impingement syndrome (31%), adhesive capsulitis (35%), and calcific tendinitis (4%). This article presents the pathophysiology, clinical characteristics, typical physical examination findings and provocation tests, and radiologic findings of common shoulder diseases, including rotator cuff disease, adhesive capsulitis, and calcific tendinitis, to provide a guide to differential diagnosis. Common shoulder diseases can be easily diagnosed with careful history taking and precise physical examination; moreover, ultrasonography is a useful diagnostic tool for rotator cuff disease and can also assist with the differential diagnosis of shoulder diseases in the outpatient clinic.
MeSH Terms
Figure
-

Figure 1 Painful arc test. (A) The patient fully elevates the arm in the scapular plane and in neutral rotation with the elbow straight. (B) And then the patient slowly lowers the arm down to the side. When the patient expressed pain between 60 and 100 degree of abduction, painful arc test is positive.

Figure 2 Neer test. The examiner places one hand on scapula to prevent scapular rotation and raises the patient's arm with the other hand in forced forward elevation, which action can cause causing the greater tuberosity to impinge against the acromion. When the patient feels pain during the motion, the test is positive.
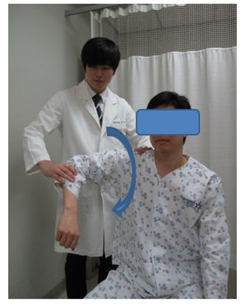
Figure 3 Hawkins-Kennedy test. The examiner places the patient's shoulder with one hand in 90 degrees of forward flexion with the elbow flexion in 90 degrees while the other hand hold the scapula. And then the examiner rotates the arm internally forcefully. The motion can cause the greater tuberosity to rotate under the acromion and coracoacromial arch, compressing the inflamed bursa and supraspinatus tendon. If the patient feels pain during internal rotation, the test is positive.

Figure 4 Empty can test (Jobe's test). The examiner assessed the deltoid with the arm at 90° of abduction and neutral rotation. And then the patient places the arm into internal rotation with forward flexion 30 degree and the thumbs toward the floor. During holding this posture the examiner pushes down at the distal forearm to test the strength of supraspinatus muscle with resistance. When there is weakness or pain provocation, the test is positive.
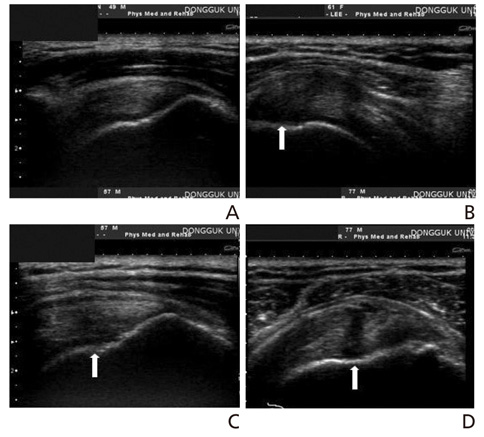
Figure 5 Ultrasonography findings in rotator cuff diseases. (A) Normal ultrasonography findings of supraspinatus tendon. Long axis view shows the hyperechoic fibrillar pattern in supraspinatus tendon. (B) Tendinosis of supraspinatus tendon. The long axis view shows diffuse swelling and hypoechoic lesion in the insertion site of supraspinatus tendon (arrow). (C) Partial thickness tear of supraspinatus tendon (articular-side). Long axis view shows focal hypoechoic lesion with loss of fibrillar pattern in articular-side of supraspinatus tendon (arrow), which is filling defect. (D) Full thickness tear of supraspinatus tendon. Long axis view shows linear fluid filled defect (arrow) throughout the articular side to bursa side of supraspinatus tendon.
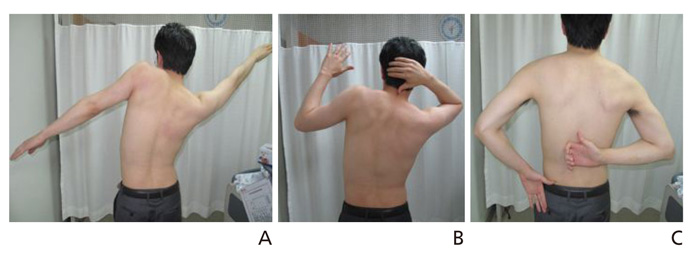
Figure 6 Shoulder active range of motion in adhesive capsulitis. (A) Stiffness of shoulder abduction is shown in left side with the rotation of scapula, which means the loss of scapulohumeral rhythm. (B) Stiffness of shoulder external rotation in left side with normal range of motion of right side. (C) Stiffness of shoulder internal rotation in left side with normal range of motion of right side.

Figure 7 Calcific tendinitis of glenohumeral joint. (A) Anteriorposterior radiography demonstrates a calcific deposition (arrow) in the supraspinatus tendon. Long axis view (B) and short axis view (C) of ultrasonography shows a hyperechoic calcific deposit with posterior shadow (arrow) in the supraspinatus tendon.
Cited by 1 articles
-
Diagnosis and non-operative treatment of shoulder pain
Shi-Uk Lee
J Korean Med Assoc. 2019;62(12):629-635. doi: 10.5124/jkma.2019.62.12.629.
Reference
-
1. Shanahan EM, Sladek R. Shoulder pain at the workplace. Best Pract Res Clin Rheumatol. 2011; 25:59–68.
Article2. National Health Insurance Service. Press release [Internet]. Seoul: National Health Insurance Service;2012. cited 2014 Jun 17. Available from: http://www.nhis.or.kr/portal/site/main/MENU_WBDCC01/.3. Seo KM, Chung SG. Upper extremity pain. In : Han TR, Bang MS, Chung SG, editors. Rehabilitation medicine. 5th ed. Seoul: Koonja Publishing;2014. p. 1032–1055.4. Greenberg DL. Evaluation and treatment of shoulder pain. Med Clin North Am. 2014; 98:487–504.
Article5. Speed C. Shoulder pain. Clin Evid. 2005; 14:1543–1560.6. Lewis JS. Rotator cuff tendinopathy. Br J Sports Med. 2009; 43:236–241.
Article7. Lee SU. Rotator cuff disease: pathology, pathophysiology, and natural course. J Korean Assoc Pain Med. 2007; 6:59–65.8. Factor D, Dale B. Current concepts of rotator cuff tendinopathy. Int J Sports Phys Ther. 2014; 9:274–288.9. Seitz AL, McClure PW, Finucane S, Boardman ND 3rd, Michener LA. Mechanisms of rotator cuff tendinopathy: intrinsic, extrinsic, or both? Clin Biomech (Bristol, Avon). 2011; 26:1–12.
Article10. Neer CS 2nd. Impingement lesions. Clin Orthop Relat Res. 1983; 173:70–77.
Article11. Park JY, Choi JH. Treatment of pain around the shoulder joint. J Korean Med Assoc. 2005; 48:1206–1214.
Article12. Tashjian RZ. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin Sports Med. 2012; 31:589–604.
Article13. Kibler WB, Murrell GA, Pluim B. Shoulder pain. In : Brunker P, Khan K, editors. Brukner & Khan's clinical sports medicine. 4th ed. New York: McGraw-Hill;2012. p. 353–376.14. Hattrup SJ, Cofield RH. Rotator cuff tears with cervical radiculopathy. J Shoulder Elbow Surg. 2010; 19:937–943.
Article15. Codsi M, McCarron J, Brems JJ. Clinical evaluation of shoulder problems. In : Rockwood CA, editor. The shoulder. 4th ed. Philadelphia: Saunders Elsevier;2009. p. 162–168.16. Jain NB, Wilcox RB 3rd, Katz JN, Higgins LD. Clinical examination of the rotator cuff. PM R. 2013; 5:45–56.
Article17. Hegedus EJ, Goode AP, Cook CE, Michener L, Myer CA, Myer DM, Wright AA. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med. 2012; 46:964–978.
Article18. Nazarian LN, Jacobson JA, Benson CB, Bancroft LW, Bedi A, McShane JM, Miller TT, Parker L, Smith J, Steinbach LS, Teefey SA, Thiele RG, Tuite MJ, Wise JN, Yamaguchi K. Imaging algorithms for evaluating suspected rotator cuff disease: Society of Radiologists in Ultrasound consensus conference statement. Radiology. 2013; 267:589–595.
Article19. Lenza M, Buchbinder R, Takwoingi Y, Johnston RV, Hanchard NC, Faloppa F. Magnetic resonance imaging, magnetic re-sonance arthrography and ultrasonography for assessing ro-tator cuff tears in people with shoulder pain for whom sur-gery is being considered. Cochrane Database Syst Rev. 2013; 9:CD009020.
Article20. Park GY. Diagnosis and rehabilitation treatment in adhesive capsulitis of the shoulder. J Korean Med Assoc. 2004; 47:1099–1106.
Article21. Robinson CM, Seah KT, Chee YH, Hindle P, Murray IR. Fro-zen shoulder. J Bone Joint Surg Br. 2012; 94:1–9.
Article22. Neviaser AS, Neviaser RJ. Adhesive capsulitis of the shoulder. J Am Acad Orthop Surg. 2011; 19:536–542.
Article23. Hannafin JA, Chiaia TA. Adhesive capsulitis. A treatment approach. Clin Orthop Relat Res. 2000; 372:95–109.24. Neviaser AS, Hannafin JA. Adhesive capsulitis: a review of current treatment. Am J Sports Med. 2010; 38:2346–2356.25. Siegal DS, Wu JS, Newman JS, Del Cura JL, Hochman MG. Calcific tendinitis: a pictorial review. Can Assoc Radiol J. 2009; 60:263–272.
Article26. Bureau NJ. Calcific tendinopathy of the shoulder. Semin Musculoskelet Radio. 2013; 17:80–84.
Article
