The Atlanto-Axial Rotatory Fixation in Adult Treated by Non-Surgical Approach
- Affiliations
-
- 1Department of Neurosurgery, Chungbuk National University School of Medicine & Medical Research Institute, Cheongju, Korea. mslee@chungbuk.ac.kr
- KMID: 2192373
- DOI: http://doi.org/10.13004/jknts.2010.6.1.70
Abstract
- The atlanto-axial rotatory fixation (AARF) is a rare clinical condition that occurs more commonly in children than in adults. It is easy to misdiagnosis AARF because of peculiar feature of atlanto-axial articulation. The authors reported a case of AARF in an adult who was treated by im-mobilization without surgery. Due to a traffic accident, the patient's head was forcefully rotated to the right side and flexed to the left side. The patient had no neurological deficit, but the patient's head was fixed in a position rotated to the right and tilted to the left. In open mouth view and three dimensional CT reconstruction images the atlas was rotated to the right side and the anterior lip of left superior facet and left transverse process of axis were fractured. The patient underwent intermittent Halter-traction for seven days. After the Halter-traction, we gained successful reduction and posterior neck pain was subsided. After the reduction, Halo-vest was applied for three months and the patient recovered well without any neurological deficits. In some case of adult traumatic AARF patient, closed reduction and Halo-vast external fixation may be successful instead of open reduction and fixation. And if it is successful, we can avoid operative procedure.
MeSH Terms
Figure
-
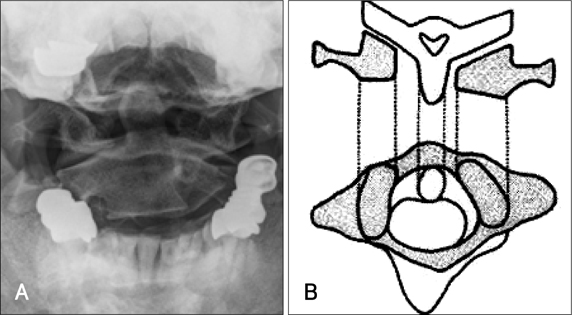
FIGURE 1 Cervical spine radiography (A) and the diagram (B) showing a abnormal position of the dens axis. A: Cervical spine open mouth radiography showed the left C1 lateral mass which is closer to the odontoid process than right one. B: Diagram of the atlas was rotated to the right compared to the axis.

FIGURE 2 Pre-reduction radiologic examination. A: Three-dimensional surface reconstructions of CT showed the atlas was rotated to right side and the anterior lip of left superior facet of C2 vertebra and left transverse process of C2 vertebra was fractured. B: Cervical spine CT revealed the atlas was rotated to the right compared to the axis. C: Cervical spine MRI revealed no evidence of cord injury.

FIGURE 3 Post-reduction radiologic examination. A: Post-reduction cervical spine open mouth radiography shows successful reduction of cervical spine. B: Follow up three-dimensional surface reconstructions of CT shows successful reduction of cervical spine (three month later). C: Follow up cervical spine CT revealed the atlas and axis has been completely corrected (three month later).
Reference
-
1. Crossman JE, Thompson D, Hayward RD, Ransford AO, Crockard HA. Recurrent atlantoaxial rotatory fixation in children: a rare complication of a rare condition. Report of four cases. J Neurosurg. 2004; 100:307–311.2. Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. (Fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. 1977; 59:37–44.
Article3. Goddard NJ, Stabler J, Albert JS. Atlanto-axial rotatory fixation and fracture of the clavicle. An association and a classification. J Bone Joint Surg Br. 1990; 72:72–75.
Article4. Jeon SW, Jeong JH, Moon SM, Choi SK. Atlantoaxial rotatory fixation in adults patient. J Korean Neurosurg Soc. 2009; 45:246–248.
Article5. Kim YS, Lee JK, Kim JH, Kim SH. Post-traumatic atlantoaxial rotatory dislocation in an adult treated by open reduction and C1-C2 transpedicular screw fixation. J Korean Neurosurg Soc. 2007; 41:248–251.
Article6. Kombogiorgas D, Hussain I, Sgouros S. Atlanto-axial rotatory fixation caused by spontaneous intracerebral haemorrhage in a child. Childs Nerv Syst. 2006; 22:1182–1186.
Article7. Leventhal MR, Maguire JK Jr, Christian CA. Christian CA. Atlantoaxial rotary subluxation in ankylosing spondylitis. A case report. Spine (Phila Pa 1976). 1990; 15:1374–1376.8. Li V, Pang D. Atlanto-axial rotatory fixation. In : Pang D, editor. Disorders of the pediatric spine. New York: Raven Press;1995. p. 531–553.9. Marar BC, Balachandran N. Non-traumatic atlanto-axial dislocation in children. Clin Orthop Relat Res. 1973; 220–226.
Article10. Munch C, Linhart W, Storck A, Papavero L, Windolf J, Rueger JM, et al. [Treatment of traumatic rotatory atlanto-axial subluxation in childhood. Case report and literature review.]. Unfallchirurg. 2005; 108:987–990.11. Rahimi SY, Stevens EA, Yeh DJ, Flannery AM, Choudhri HF, Lee MR. Treatment of atlantoaxial instability in pediatric patients. Neurosurg Focus. 2003; 15:ECP1.
Article12. Rinaldi I, Mullins WJ Jr, Delaney WF, Fitzer PM, Tornberg DN. Computerized tomographic monstration of rotational atlanto-axial fixation. J Neurosurg. 1979; 50:115–119.13. Roche CJ, O'Malley M, Dorgan JC, Carty HM. pictorial review of atlanto-axial rotatory fixation: key points for the radiologist. Clin Radiol. 2001; 56:947–958.14. Sohn MJ, Rhim SC, Roh SW, Park HC. Atlantoaxial rotatory fixation: report of 3 cases. J Korean Neurosurg Soc. 2000; 29:580–585.15. Taddonio RF Jr, King AG. Atlantoaxial rotatory fixation after decompressive laminectomy. A case report. Spine (Phila Pa 1976). 1982; 7:540–554.16. White GM, Healy WL. Tumor-associated atlanto-axial rotatory fixation. A case report. Spine (Phila Pa 1976). 1987; 12:406–408.17. Wortzman G, Dewar FP. Rotatory fixation of the atlantoaxial joint: rotational atlantoaxial subluxation. Radiology. 1968; 90:479–487.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atlanto-Axial Rotatory Fixation: Report of A Case
- Traumatic Atlanto-Occipital Rotatory Posterior Dislocation Combined with Atlanto-Axial Rotatory Subluxation: A Case Report
- Non-traumatic Atlanto-axial Rotatory Subluxation: A Case Report
- Transoral Approach of Atlanto-Axial Pyogenic Abscess
- Combined Atlantoaxial Rotatory Fixation and Unilateral Counter Occipitoatlantal Subluxation after Minor Trauma
