J Korean Neurotraumatol Soc.
2010 Jun;6(1):53-56. 10.13004/jknts.2010.6.1.53.
Clinical Application of the Calcium Phosphate Cement (PolyBone(R)) for the Skull Bone Defects after Microvascular Decompression
- Affiliations
-
- 1Department of Neurosurgery, Yeouido ST' Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. rhalee@catholic.ac.kr
- KMID: 2192367
- DOI: http://doi.org/10.13004/jknts.2010.6.1.53
Abstract
OBJECTIVE
Skull bone defects after microvascular decompression (MVD) were usually troublesome to the patients and surgeons. Recently, the use of calcium phosphate cements has become more common in craniofacial surgery because of several advantages. We retrospectively studied clinical usefulness of newly developed calcium phosphate cements (PolyBone(R), Kyeung-won med., Seoul, Korea) in cranial reconstruction after MVD operation.
METHODS
From January 2007 to December 2008 we performed retrosigmoid craniotomy in 20 patients with trigeminal neuralgia or hemifacial spasm. Calcium phosphate cements was used as a bone mineral substitute to repair the surgically induced bone defects in cranium.
RESULTS
Mean follow up period was 12.15+/-4.35 months. There was no inflammatory reaction surrounding the implanted materials and no air or cerebrospinal fluid leakage. Postoperative plain x-ray of skull showed good healing and shaping of suboccipital bone at the surgical defect in all patients. The material could be seen as a dense, radio-opaque structure without the material artifacts.
CONCLUSION
We have demonstrated calcium phosphate cement is useful to repair and augment the surgically induced bone defects for cranio-facial surgery especially for small defects of the after MVD.
MeSH Terms
Figure
-
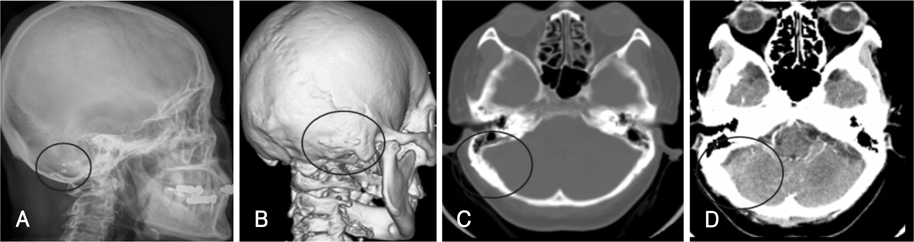
FIGURE 1 Post operative radiologic findings after reconstructive surgery. A: Postoperative X-ray shows bone flap fixed by screws and plates and filling with calcium phosphate cement (Polybone®, Kyeung-won med., Seoul, Korea) polybone at the defect site. B: Three-dimensional CT scan at 3 months after surgery shows no bony defect. C: Postoperative bone setting CT. Calcium phosphate cement integrated with bone flap and defected site. The margin between bone flap and defected site is not obvious. D: The enhanced CT shows no definite abnormal enhancement around the operation site.
Reference
-
1. Ambard AJ, Mueninghoff L. Calcium phosphate cement: review of mechanical and biological properties. J Prosthodont. 2006; 15:321–328.
Article2. Britz GW, Vilela MD, Futran N, Rostomily R. Cosmetic concerns in posterior fossa skull base surgery. Neurosurg Clin N Am. 2002; 13:475–489.
Article3. Elkins CW, Cameron JE. Cranioplasty with acrylic plates. J Neurosurg. 1946; 3:199–205.
Article4. Imola MJ, Sciarretta V, Schramm VL. Skull base reconstruction. Curr Opin Otolaryngol Head Neck Surg. 2003; 11:282–290.
Article5. Ishikawa K, Asaoka K. Estimation of ideal mechanical strength and critical porosity of calcium phosphate cement. J Biomed Mater Res. 1995; 29:1537–1543.
Article6. Le Nihouannen D, Komarova SV, Gbureck U, Barralet JE. Bioactivity of bone resorptive factor loaded on osteoconductive matrices: stability post-dehydration. Eur J Pharm Biopharm. 2008; 70:813–818.
Article7. Lovely TJ, Lowry DW, Jannetta PJ. Functional outcome and the effect of cranioplasty after retromastoid craniectomy for microvascular decompression. Surg Neurol. 1999; 51:191–197.
Article8. McLaughlin MR, Jannetta PJ, Clyde BL, Subach BR, Comey CH, Resnick DK. Microvascular decompression of cranial nerves: lessons learned after 4400 operations. J Neurosurg. 1999; 90:1–8.
Article9. Park JS, Kong DS, Lee JA, Park K. Intraoperative management to prevent cerebrospinal fluid leakage after microvascular decompression: dural closure with a "plugging muscle" method. Neurosurg Rev. 2007; 30:139–142. discussion 142.
Article10. Sahoo N, Ray ID, Desai AP, Gupta V. Comparative evaluation of autogenous calvarial bone graft and alloplastic materials for secondary reconstruction of cranial defects. J Craniofac Surg. 2010; 21:79–82.
Article11. Samii M, Günther T, Iaconetta G, Muehling M, Vorkapic P, Samii A. Microvascular decompression to treat hemifacial spasm: longterm results for a consecutive series of 143 patients. Neurosurgery. 2002; 50:712–718. discussion 718-719.
Article12. Sanan A, Haines SJ. Repairing holes in the head a history of cranioplasty. Neurosurgery. 1997; 40:588–603.
Article13. Schessel DA, Rowed DW, Nedzelski JM, Feghali JG. Postoperative pain following excision of acoustic neuroma by the suboccipital approach: observations on possible cause and potential amelioration. Am J Otol. 1993; 14:491–494.
Article14. Takechi M, Miyamoto Y, Ishikawa K, Toh T, Yuasa T, Nagayama M, et al. Initial histological evaluation of anti-washout type fast-setting calcium phosphate cement following subcutaneous implantation. Biomaterials. 1998; 19:2057–2063.
Article15. Yamaki T, Odake G, Horikawa Y, Suzuki K, Fujimoto M, Naruse S, et al. [Clinical and experimental study of heart-cured methyl methacrylate for cranioplasty (author's transl).]. Neurol Med Chir (Tokyo). 1978; 18:323–329.16. Yamashima T. Reconstruction of surgical skull defects with hydroxylapatite ceramic buttons and granules. Acta Neurochir (Wien). 1988; 90:157–162.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Experience of the Brushite Calcium Phosphate Cement for the Repair and Augmentation of Surgically Induced Cranial Defects Following the Pterional Craniotomy
- The experimental study of the effect of zinc phosphate cement on the solubility of enamel
- Successful Bone Union Following Calcium Phosphate Cement-Assisted Percutaneous Transpedicular Balloon Kyphoplasty of a Large Interbody Cleft on Long-term Hemodialysis Patient
- The effects of novel biodegradable amorphous Calcium Phosphate on bone regeneration in rat calvarial defects
- Histometrical evaluation of biphasic calcium phosphate in surgically created 1-wall periodontal intrabony defects in dogs
