A Large Ruptured Anterior Communicating Artery Aneurysm Presenting with Bitemporal Hemianopsia
- Affiliations
-
- 1Department of Neurosurgery, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea. ysparkns@kosinmed.or.kr
- KMID: 2191386
- DOI: http://doi.org/10.3340/jkns.2015.58.3.291
Abstract
- Anterior communicating artery (ACoA) aneurysms sometimes present with visual symptoms when they rupture or directly compress the optic nerve. Giant or large ACoA aneurysms producing bitemporal hemianopsia are extremely rare. Here we present an unusual case of bitemporal hemianopsia caused by a large intracranial aneurysm of the ACoA. A 41-year-old woman was admitted to our neurosurgical department with a sudden-onset bursting headache and visual impairment. On admission, her vision was decreased to finger counting at 30 cm in the left eye and 50 cm in the right eye, and a severe bitemporal hemianopsia was demonstrated on visual field testing. A brain computed tomography scan revealed a subarachnoid hemorrhage at the basal cistern, and conventional cerebral catheter angiography of the left internal carotid artery demonstrated an 18x8 mm dumbbell-shaped aneurysm at the ACoA. Microscopic aneurysmal clipping was performed. An ACoA aneurysm can produce visual field defects by compressing the optic chiasm or nerves. We emphasize that it is important to diagnose an aneurysm through cerebrovascular study to prevent confusing it with pituitary apoplexy.
Keyword
MeSH Terms
Figure
-
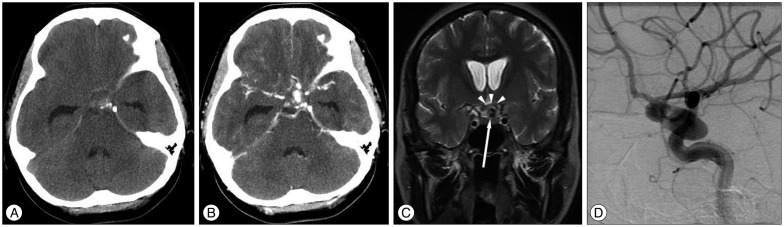
Fig. 1 Brain computed tomography scan shows a subarachnoid hemorrhage at the basal cistern (A) and a oval lesion with contrast filling at the sellar region (B). Brain magnetic resonance imaging shows the optic chiasm (arrow heads) deviating upward by the aneurysm (arrow) (C). Cerebral catheter angiography in the left internal carotid artery demonstrates an 18×8 mm dumbbell-shaped aneurysm at the anterior communicating artery (D).

Fig. 2 Intra-operative view shows an aneurysmal sac on the anterior border of the optic chiasm (A). A large aneurysm grows forward and downward in the front of the free edge of the chiasm and pushes the chiasm upward and backward (*). Postoperative cerebral catheter angiography demonstrates complete occlusion of the aneurysmal sac by a clip (B). AN : aneurysm, ICA : internal carotid artery, ON : optic nerve.
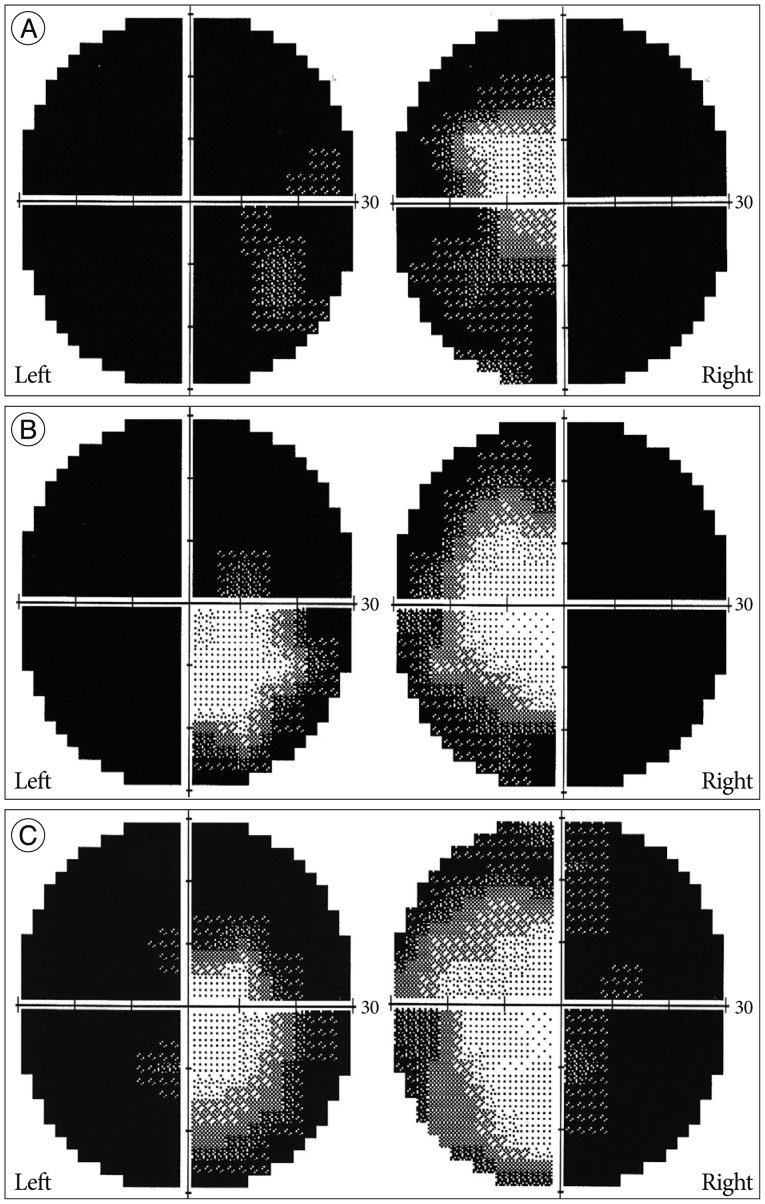
Fig. 3 The patient underwent perimetry testing three times at postoperative 3 days (A), 15 days (B), and 9 months (C). The patient's visual acuity and field were slightly improved during 9 months after surgery.
Reference
-
1. Aoki N. Partially thrombosed aneurysm presenting as the sudden onset of bitemporal hemianopsia. Neurosurgery. 1988; 22:564–566. PMID: 3362325.
Article2. Chan JW, Hoyt WF, Ellis WG, Gress D. Pathogenesis of acute monocular blindness from leaking anterior communicating artery aneurysms : report of six cases. Neurology. 1997; 48:680–683. PMID: 9065547.
Article3. Claes C, Milea D, Bodaghi B, Tran TH, LeHoang P, Blanc R. Acute retrobulbar optic neuropathy due to rupture of an anterior communicating artery aneurysm. Acta Ophthalmol Scand. 2006; 84:145–146. PMID: 16445456.
Article4. Date I, Akioka T, Ohmoto T. Penetration of the optic chiasm by a ruptured anterior communicating artery aneurysm. Case report. J Neurosurg. 1997; 87:324–326. PMID: 9254100.
Article5. Ferguson GG, Drake CG. Carotid-ophthalmic aneurysms : visual abnormalities in 32 patients and the results of treatment. Surg Neurol. 1981; 16:1–8. PMID: 7280963.
Article6. Hara N, Mukuno K, Ohtaka H, Shimizu K. Ischemic optic neuropathy associated with subarachnoid hemorrhage after rupture of anterior communicating artery aneurysm. Ophthalmologica. 2003; 217:79–84. PMID: 12566879.
Article7. Højer-Pedersen E, Haase J. Giant anterior communicating artery aneurysm with bitemporal hemianopsia : case report. Neurosurgery. 1981; 8:703–706. PMID: 7279157.
Article8. Jefferson G. Further concerning compression of the optic pathways by intracranial aneurysms. Clin Neurosurg. 1953; 1:55–103. PMID: 14379465.
Article9. Koo SK, Song YJ, Huh JT. Surgically treated anterior communicating artery aneurysm. J Korean Neurosurg Soc. 2005; 37:405–409.10. Moller PM, Hvid-Hansen O. Chiasmal visual fields. Acta Ophthalmol (Copenh). 1970; 48:678–684. PMID: 5536714.11. Nishino A, Sakurai Y, Arai H, Nishimura S, Suzuki S, Uenohara H. Clinical manifestations, character of aneurysms, and surgical results for unruptured cerebral aneurysms presenting with ophthalmic symptoms. Acta Neurochir Suppl. 2002; 82:47–49. PMID: 12378990.
Article12. Norwood EG, Kline LB, Chandra-Sekar B, Harsh GR 3rd. Aneurysmal compression of the anterior visual pathways. Neurology. 1986; 36:1035–1041. PMID: 3736868.
Article13. Park JH, Park SK, Kim TH, Shin JJ, Shin HS, Hwang YS. Anterior communicating artery aneurysm related to visual symptoms. J Korean Neurosurg Soc. 2009; 46:232–238. PMID: 19844624.
Article14. Peiris JB, Ross Russell RW. Giant aneurysms of the carotid system presenting as visual field defect. J Neurol Neurosurg Psychiatry. 1980; 43:1053–1064. PMID: 7217950.
Article15. Ruben S, Afshar F. Visual failure following subarachnoid haemorrhage from rupture of an anterior communicating artery aneurysm. J Neurol Neurosurg Psychiatry. 1991; 54:1017–1018. PMID: 1800651.
Article16. Schisano G. Large anterior communicating artery aneurysm with temporal hemianopsia. Case report. J Neurosurg Sci. 1985; 29:267–271. PMID: 3831272.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subdural Hematoma Due to Ruptured Intracerebral Aneurysm
- An Unruptured Anterior Communicating Artery Aneurysm Presenting with Left Homonymous Hemianopsia: A Case Report
- Ruptured proximal anterior cerebral artery (A1) aneurysm located at an anomalous branching of the fronto-orbital artery--a case report
- Microsurgical anatomy of the Anterior Cerebral-anterior Communicating Artery
- Giant Serpentine Aneurysm of the Anterior Communicating Artery: Case Report
