Usefulness of Intraoperative Monitoring during Microsurgical Decompression of Cervicomedullary Compression Caused by an Anomalous Vertebral Artery
- Affiliations
-
- 1Department of Neurosurgery, Busan Paik Hospital, Inje University School of Medicine, Busan, Korea. 106304@paik.ac.kr
- KMID: 2191148
- DOI: http://doi.org/10.3340/jkns.2014.56.6.513
Abstract
- We report a case of cervicomedullary compression by an anomalous vertebral artery treated using microsurgical decompression with intraoperative monitoring. A 68-year-old woman presented with posterior neck pain and gait disturbance. MRI revealed multiple abnormalities, including an anomalous vertebral artery that compressed the spinal cord at the cervicomedullary junction. Suboccipital craniectomy with C1 laminectomy was performed. The spinal cord was found to be compressed by the vertebral arteries, which were retracted dorsolaterally. At that time, the somatosensory evoked potential (SSEP) changed. After release of the vertebral artery, the SSEP signal normalized instantly. The vertebral artery was then lifted gently and anchored to the dura. There was no other procedural complication. The patient's symptoms improved. This case demonstrates that intraoperative monitoring may be useful for preventing procedural complications during spinal cord microsurgical decompression.
Keyword
MeSH Terms
Figure
-
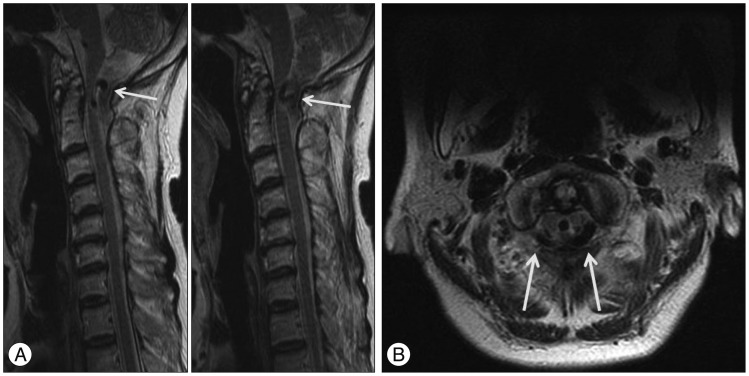
Fig. 1 Sagittal T2-weighted MR images of the cervical spine (A) show the anomalous vertebral arteries (arrows) located dorsal to the spinal cord. Axial T2-weighted MR image of the C1 level (B) shows the anomalous tortuous vertebral arteries (arrows) that compressed the dorsal portion of the spinal cord bilaterally at the cervicomedullary junction. Neither congenital anomalies of the posterior fossa nor any degenerative changes to the spinal column were evident.
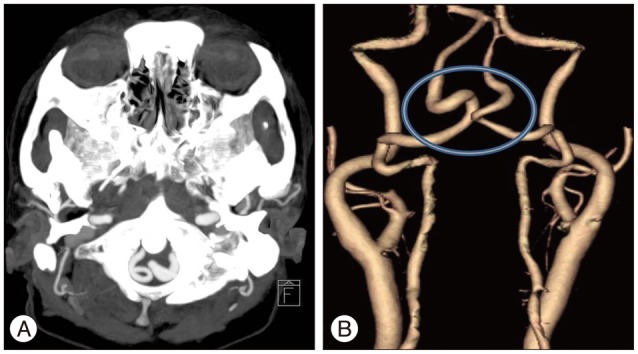
Fig. 2 CT angiography source image (A) and 3D reconstructed image (B) revealed that both vertebral arteries were elongated and enlarged. The hollow indicates the intradural segment of the elongated and enlarged vertebral arteries.
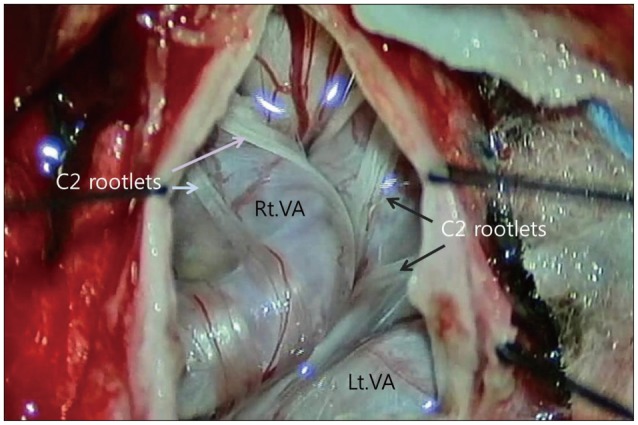
Fig. 3 Intraoperative photograph, showing the dura opened into a Y shape, and the elongated and enlarged vertebral arteries (VAs) that seemed somewhat sclerotic. Both the VAs were kissing each other. The C2 rootlets (arrows) were entangled in the VAs.
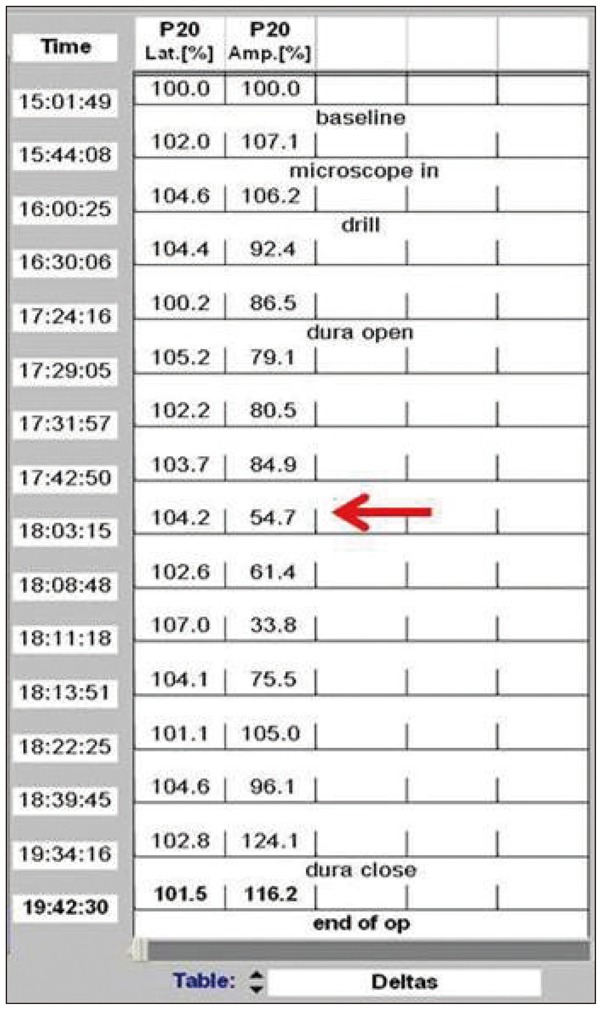
Fig. 4 Amplitude of the somatosensory evoked potential for the right tibialis anterior muscle dropped below 50% of baseline during the operation (red arrow).
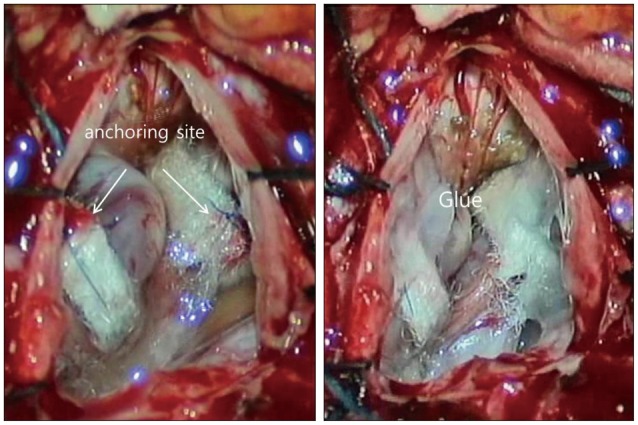
Fig. 5 Both the vertebral arteries were anchored to the dura (arrow) using Teflon slings and silk sutures. Following that, the area was bonded using surgical glue.
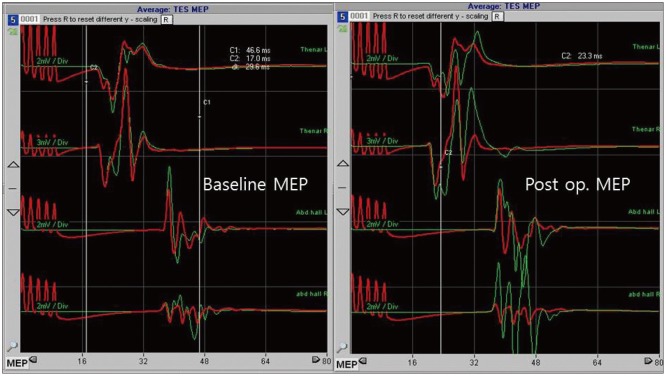
Fig. 6 An increase in the motor evoked potentials was noted after dura closure, compared to the baseline values.
Reference
-
1. Aryanpur J, Hurko O, Francomano C, Wang H, Carson B. Craniocervical decompression for cervicomedullary compression in pediatric patients with achondroplasia. J Neurosurg. 1990; 73:375–382. PMID: 2384775.
Article2. Ball BG, Krueger BR, Piepgras DG. Anomalous vertebral artery compression of the spinal cord at the cervicomedullary junction. Surg Neurol Int. 2011; 2:103. PMID: 21886876.
Article3. Deletis V, Sala F. Intraoperative neurophysiological monitoring of the spinal cord during spinal cord and spine surgery : a review focus on the corticospinal tracts. Clin Neurophysiol. 2008; 119:248–264. PMID: 18053764.
Article4. Detwiler PW, Porter RW, Harrington TR, Sonntag VK, Spetzler RF. Vascular decompression of a vertebral artery loop producing cervical radiculopathy. Case report. J Neurosurg. 1998; 89:485–488. PMID: 9724128.
Article5. Furumoto T, Nagase J, Takahashi K, Itabashi T, Iai H, Ishige N. Cervical myelopathy caused by the anomalous vertebral artery. A case report. Spine (Phila Pa 1976). 1996; 21:2280–2283. PMID: 8902976.6. Grabb PA, Mapstone TB, Oakes WJ. Ventral brain stem compression in pediatric and young adult patients with Chiari I malformations. Neurosurgery. 1999; 44:520–527. discussion 527-528. PMID: 10069589.
Article7. Jamjoom AB, Rawlinson JN, Coakham HB. Multiple neurological lesions due to vertebrobasilar dolichoectasia. Br J Neurosurg. 1990; 4:147–154. PMID: 2357284.
Article8. Kim K, Mizunari T, Kobayashi S, Ishii S, Teramoto A. [Occipital neuralgia caused by the compression of the fenestrated vertebral artery: a case report]. No Shinkei Geka. 1999; 27:645–650. PMID: 10440039.9. Kitagawa M, Nakagawa Y, Kitaoka K, Kobayashi N, Ishikawa T, Nagashima M. [Accessory nerve paralysis due to compression of the fenestrated vertebral artery]. No Shinkei Geka. 1988; 16:1173–1177. PMID: 3205359.10. Kothbauer KF. Intraoperative neurophysiologic monitoring for intramedullary spinal-cord tumor surgery. Neurophysiol Clin. 2007; 37:407–414. PMID: 18083496.
Article11. Koyama S, Maeda T, Komine A. [Medulla and upper cervical cord compression by bilateral vertebral artery presented with myelopathy and drop attack: case report]. No To Shinkei. 2002; 54:435–439. PMID: 12058415.12. Maiuri F, Iaconetta G, Gallicchio B, Briganti F. Coiling of the vertebral artery presenting with neuralgic pain. Clin Neurol Neurosurg. 1997; 99:56–59. PMID: 9107470.
Article13. Morikawa K, Ohkawa N, Yamashita S. [Surgical decompression for the C-1 and C-2 sensory roots and upper cervical cord in a case with cervical myelopathy and occipital neuralgia due to bilateral fenestration of vertebral artery: a case report]. No Shinkei Geka. 1993; 21:1035–1038. PMID: 8255379.14. Nash CL Jr, Lorig RA, Schatzinger LA, Brown RH. Spinal cord monitoring during operative treatment of the spine. Clin Orthop Relat Res. 1977; (126):100–105. PMID: 598095.
Article15. Nishiura T, Fujiwara K, Handa A, Gotoh M, Tsuno K, Ishimitsu H. [Cervical myelopathy caused by bilateral vertebral artery compression]. No Shinkei Geka. 1998; 26:45–50. PMID: 9488991.16. Paksoy Y, Levendoglu FD, Ogün CO, Ustün ME, Ogün TC. Vertebral artery loop formation a frequent cause of cervicobrachial pain. Spine (Phila Pa 1976). 2003; 28:1183–1188. PMID: 12782990.
Article17. Pico F, Labreuche J, Touboul PJ, Amarenco P. GENIC Investigators. Intracranial arterial dolichoectasia and its relation with atherosclerosis and stroke subtype. Neurology. 2003; 61:1736–1742. PMID: 14694039.
Article18. Riew KD, Raich AL, Dettori JR, Heller JG. Neck Pain Following Cervical Laminoplasty : Does Preservation of the C2 Muscle Attachments and/or C7 Matter? Evid Based Spine Care J. 2013; 4:42–53. PMID: 24436698.19. Sakaura H, Hosono N, Mukai Y, Fujimori T, Iwasaki M, Yoshikawa H. Preservation of muscles attached to the C2 and C7 spinous processes rather than subaxial deep extensors reduces adverse effects after cervical laminoplasty. Spine (Phila Pa 1976). 2010; 35:E782–E786. PMID: 20581755.
Article20. Satoh S, Yamamoto N, Kitagawa Y, Umemori T, Sasaki T, Iida T. Cervical cord compression by the anomalous vertebral artery presenting with neuralgic pain. Case report. J Neurosurg. 1993; 79:283–285. PMID: 8331414.
Article21. Shah A, Mahore A, Goel A. Bilateral vasculopexy of anomalous vertebral arteries causing cervicomedullary compression : case report and technical note. Eur Spine J. 2012; 21(Suppl):S505–S508. PMID: 22237850.22. Smoker WR, Price MJ, Keyes WD, Corbett JJ, Gentry LR. High-resolution computed tomography of the basilar artery : 1. Normal size and position. AJNR Am J Neuroradiol. 1986; 7:55–60. PMID: 3082144.23. Takahashi Y, Sugita S, Uchikado H, Miyagi T, Tokutomi T, Shigemori M. Cervical myelopathy due to compression by bilateral vertebral arteries--case report. Neurol Med Chir (Tokyo). 2001; 41:322–324. PMID: 11458746.
Article24. Takei H, Sagae M, Chiba K, Ogino T. The long-term follow-up of surgical treatment for cervical myelopathy with severe nape and upper arm pain caused by the anomalous vertebral artery : case report. Spine (Phila Pa 1976). 2008; 33:E611–E613. PMID: 18670330.25. Ubogu EE, Chase CM, Verrees MA, Metzger AK, Zaidat OO. Cervicomedullary junction compression caused by vertebral artery dolichoectasia and requiring surgical treatment. Case report. J Neurosurg. 2002; 96:140–143. PMID: 11794596.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cervical Compressive Myelopathy due to Anomalous Bilateral Vertebral Artery
- Cervicogenic Vertigo Treated by C1 Transverse Foramen Decompression : A Case Report
- Anomalous Origin of the Vertebral Artery From the Internal Carotid Artery
- Iatrogenic Vertebral Artery Injury During Anterior Cervical Spine Surgery : Report of Two Cases
- Rotational Vertebral Artery Compression : Bow Hunter's Syndrome
