Minimally Invasive Removal of an Intradural Cervical Tumor : Assessment of a Combined Split-Spinous Laminectomy and Quadrant Tube Retractor System Technique
- Affiliations
-
- 1Department of Neurosurgery, Kyungpook National University Hospital, Daegu, Korea. nskimkt7@gmail.com
- 2Department of Neurosurgery, College of Medicine, Chung-Ang University, Seoul, Korea.
- KMID: 2190667
- DOI: http://doi.org/10.3340/jkns.2012.52.4.427
Abstract
- Conventional laminectomy is the most popular technique for the complete removal of intradural spinal tumors. In particular, the central portion intramedullary tumor and large intradural extramedullary tumor often require a total laminectomy for the midline myelotomy, sufficient decompression, and adequate visualization. However, this technique has the disadvantages of a wide incision, extensive periosteal muscle dissection, and bony structural injury. Recently, split-spinous laminectomy and tubular retractor systems were found to decrease postoperative muscle injuries, skin incision size and discomfort. The combined technique of split-spinous laminectomy, using a quadrant tube retractor system allows for an excellent exposure of the tumor with minimal trauma of the surrounding tissue. We propose that this technique offers possible advantages over the traditional open tumor removal of the intradural spinal cord tumors, which covers one or two cervical levels and requires a total laminectomy.
Figure
-
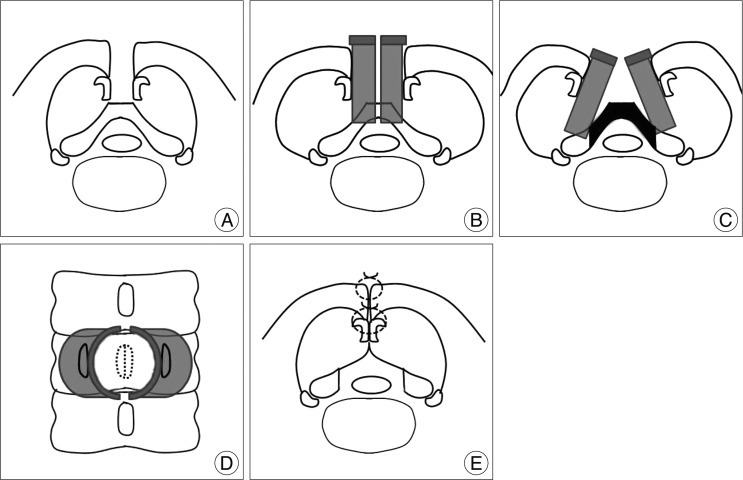
Fig. 1 Schematic drawing of the combined split-spinous laminectomy and quadrant tube retractor system technique. A : Split-spinous process and spinous process divided at its base, preserving the paraspinalis muscles attachments. B : Quadrant tube retractors are placed on the exposed lamina with a slight opening. C : Quadrant tube retractors are wide enough for total laminectomy. The black region is required for a total laminectomy. D : Operator's view of C. E : Each half of the split-spinous process is re-approximated after successful tumor removal.
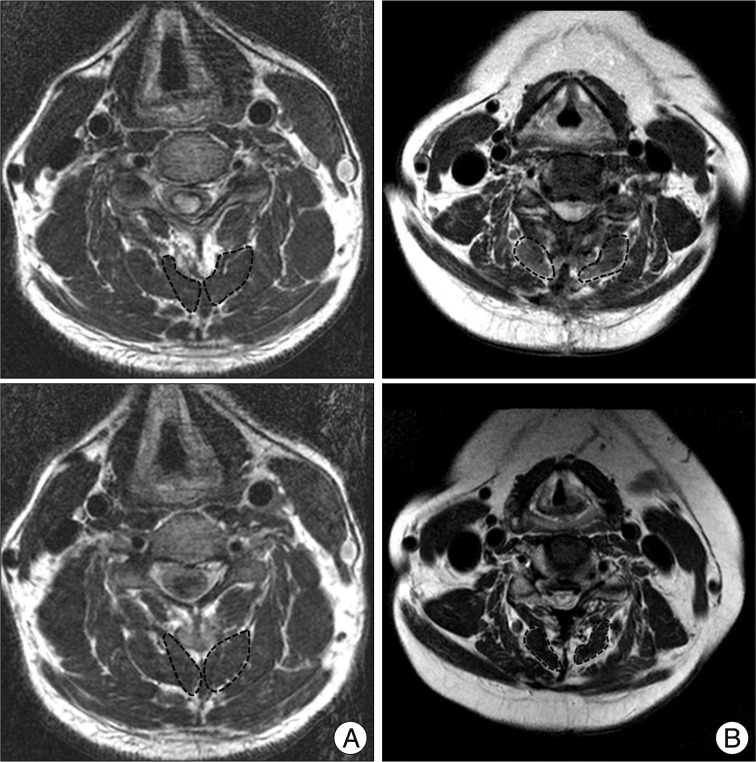
Fig. 2 Preoperative and two-year postoperative T2-weighted axial MR images. The dotted lines outline the deep extensor muscles margins. A : Combined split-spinous laminectomy and quadrant tube retractor system technique, with a muscle atrophy rate of 13% (A1 : preoperative MRI, A2 : postoperative MRI). B : Conventional total laminectomy technique, with a muscle atrophy rate of 54% (B1 : preoperative MRI, B2 : postoperative MRI).
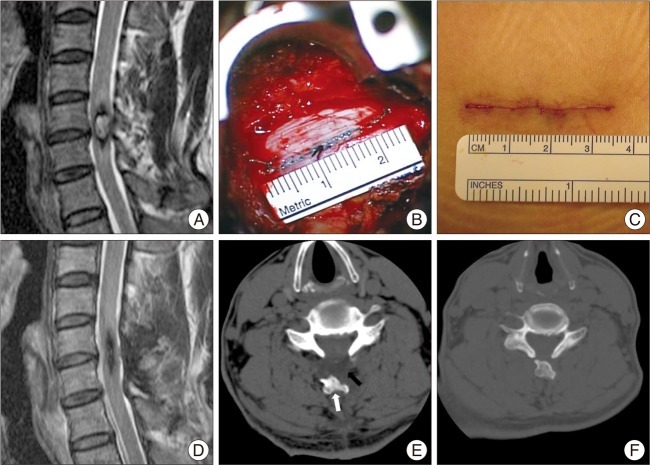
Fig. 3 Central cavernous hemangioma. A : Preoperative T2-weighted sagittal MRI showing a centrally located intramedullary tumor. B : Intraoperative image showing meticulous dural closure in quadrant tube retractors. C : This figure showing a skin closure after removing of retractors. D : Two-year postoperative T2-weighted sagittal MRI showing no evidence of tumor recurrence. E : Postoperative one-month CT showing focal fluid collection (black arrow) and deviatory split spinous process (white arrow). F : Two-year postoperative CT showing resolved fluid collection and proper location of the spinous process with complete bony fusion.
Reference
-
1. Banczerowski P, Vajda J, Veres R. Exploration and decompression of the spinal canal using split laminotomy and its modification, the "archbone" technique. Neurosurgery. 2008; 62:ONS432–ONS440. discussion ONS440-ONS441. PMID: 18596526.
Article2. Foley KT, Smith MM, Rampersaud YR. Microendoscopic approach to far-lateral lumbar disc herniation. Neurosurg Focus. 1999; 7:e5. PMID: 16918212.
Article3. Hida S, Naito M, Arimizu J, Morishita Y, Nakamura A. The transverse placement laminoplasty using titanium miniplates for the reconstruction of the laminae in thoracic and lumbar lesion. Eur Spine J. 2006; 15:1292–1297. PMID: 16612643.
Article4. Kim KT, Kim YB. Comparison between open procedure and tubular retractor assisted procedure for cervical radiculopathy : results of a randomized controlled study. J Korean Med Sci. 2009; 24:649–653. PMID: 19654947.
Article5. Kurokawa T, Tsuyama N, Tanaka H. Enlargement of spinal canal by the sagittal splitting of the spinous process. Bessatsu Seikeigeka. 1982; 2:234–240.6. Lee DY, Lee SH. Spinous process splitting laminectomy for lumbar canal stenosis : a critical appraisal. Minim Invasive Neurosurg. 2008; 51:204–207. PMID: 18683110.
Article7. Levy WJ, Latchaw J, Hahn JF, Sawhny B, Bay J, Dohn DF. Spinal neurofibromas : a report of 66 cases and a comparison with meningiomas. Neurosurgery. 1986; 18:331–334. PMID: 3084994.
Article8. Nolan JP Jr, Sherk HH. Biomechanical evaluation of the extensor musculature of the cervical spine. Spine (Phila Pa 1976). 1988; 13:9–11. PMID: 3381146.
Article9. Oktem IS, Akdemir H, Kurtsoy A, Koç RK, Menkü A, Tucer B. Hemilaminectomy for the removal of the spinal lesions. Spinal Cord. 2000; 38:92–96. PMID: 10762181.
Article10. Seppälä MT, Haltia MJ, Sankila RJ, Jääskeläinen JE, Heiskanen O. Long-term outcome after removal of spinal schwannoma : a clinicopathological study of 187 cases. J Neurosurg. 1995; 83:621–626. PMID: 7674010.
Article11. Shiraishi T. Skip laminectomy--a new treatment for cervical spondylotic myelopathy, preserving bilateral muscular attachments to the spinous processes : a preliminary report. Spine J. 2002; 2:108–115. PMID: 14588269.
Article12. Tredway TL, Santiago P, Hrubes MR, Song JK, Christie SD, Fessler RG. Minimally invasive resection of intradural-extramedullary spinal neoplasms. Neurosurgery. 2006; 58:ONS52–ONS58. discussion ONS52-ONS58. PMID: 16479629.
Article13. Watanabe K, Hosoya T, Shiraishi T, Matsumoto M, Chiba K, Toyama Y. Lumbar spinous process-splitting laminectomy for lumbar canal stenosis. Technical note. J Neurosurg Spine. 2005; 3:405–408. PMID: 16302638.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Applications of the Tubular Retractor on Spinal Disorders
- Removal of Intradural-Extramedullary Spinal Cord Tumors with Unilateral Limited Laminectomy
- A Minimally Invasive Lumbar Spine Surgery Technique Using a Modified Thoracoport: Proposal of a New Tubular Retractor
- Spinous Process-Splitting Hemilaminoplasty for Intradural and Extradural Lesions
- Unilateral Laminectomy and Bilateral Decompression for Lumbar Spinal Stenosis with Microscope and Tubular Retractor System
