Spinous Process-Splitting Hemilaminoplasty for Intradural and Extradural Lesions
- Affiliations
-
- 1Department of Neurological Surgery, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea.
- 2Department of Neurosurgery, Chung-Ang University College of Medicine, Seoul, Korea. ybkim1218@cau.ac.kr
- KMID: 2191420
- DOI: http://doi.org/10.3340/jkns.2015.58.5.494
Abstract
OBJECTIVE
To describe a novel spinous process-splitting hemilaminoplasty technique for the surgical treatment of intradural and posterior epidural lesions that promotes physiological restoration.
METHODS
The spinous process was split, the area of the facet lamina junction was drilled, and en bloc hemilaminectomy was then performed. After removing intradural and posterior epidural lesions, we fitted the previously en bloc-removed bone to the pre-surgery same shape, and held it in place with non-absorbable sutures. Surgery was performed on 16 laminas from a total of nine patients between 2011 and 2014. Bony union of the reconstructed lamina was assessed using computed tomography (CT) at 6 months after surgery.
RESULTS
Spinous process-slitting hemilaminoplasty was performed for intradural extramedullary tumors in eight patients and for ossification of the ligament flavum in one patient. Because we were able to visualize the margin of the ipsilateral and contralateral dura, we were able to secure space for removal of the lesion and closure of the dura. None of the cases showed spinal deformity or other complications. Bone fusion and maintenance of the spinal canal were found to be perfect on CT scans.
CONCLUSION
The spinous process-splitting hemilaminoplasty technique presented here was successful in creating sufficient space to remove intradural and posterior epidural lesions and to close the dura. Furthermore, we were able to maintain the physiological barrier and integrity after surgery because the posterior musculature and bone structures were restored.
Keyword
Figure
-
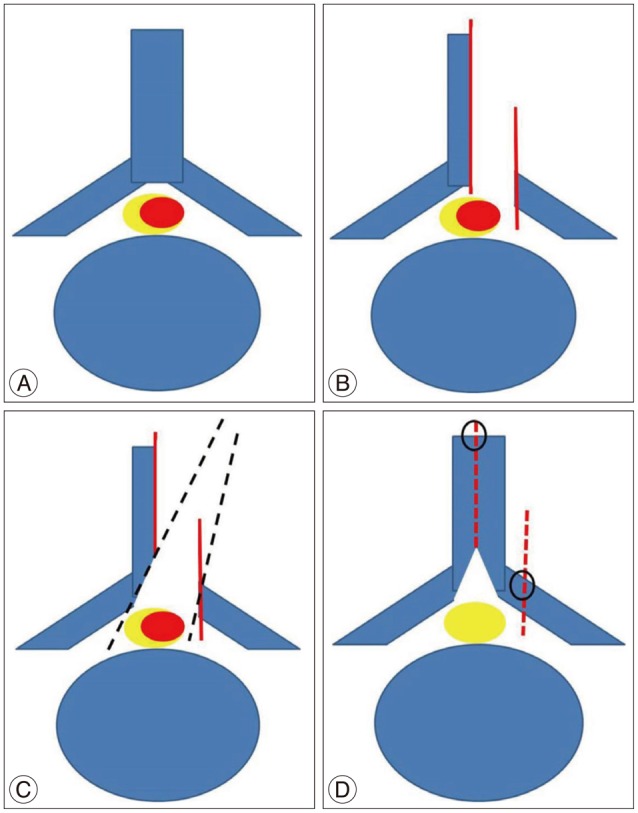
Fig. 1 A : Intradural spinal lesion (red). B : hemilaminectomy after splitting of the spinous process (using ossillating saw or T-saw) and laminofacet jounction (using match head burr). C : Contralateral spinolamina junction undercutting and exposure contralateral dural margin. D : Removal intraldural lesions and performed hemilaminoplasty.

Fig. 2 Case 1. A 57-year-old woman with an intradural extramedullary schwannoma at C3-4-5. Preoperative gadolinium-enhanced T1-weighted magnetic resonance imaging, where the sagittal and axial images reveal a left-sided intradural extramedullary lesion (A and B). Computed tomography scans obtained immediately after surgery (C) and 6 months after spinous process-splitting hemilaminoplasty (C3-4-5) (D), suggesting complete bone fusion.

Fig. 3 Case 5. A 55-year-old man with a schwannoma. A : Preoperative T2-weighted axial magnetic resonance image. B : Preoperative axial computed tomography image. The tumor was completely removed via spinous process-splitting hemilaminoplasty at L1. C : Computed tomography scans obtained immediately after the laminoplasty.

Fig. 4 Case 5. Intraoperative image. A : While performing spinous process-splitting laminectomy, the dura on both sides was visible. B : A width of approximately 1 cm was available for surgical entry.

Fig. 5 Case 7. A 62-year-old woman with cervical schwannoma. A : Preoperative T2-weighted axial magnetic resonance image. B : Preoperative axial magnetic resonance image. C : Computed tomography scans obtained immediately after the laminoplasty.
Reference
-
1. Asazuma T, Yamagishi M, Sato M, Ichimura S, Fujikawa K. Vertebral arch reconstruction based on 90 degree rotational laminoplasty after removal of spinal cord and cauda equina tumours. Acta Neurochir (Wien). 2003; 145:495–500. discussion 500PMID: 12836075.
Article2. Balak N. Unilateral partial hemilaminectomy in the removal of a large spinal ependymoma. Spine J. 2008; 8:1030–1036. PMID: 17938003.
Article3. Hara M, Takayasu M, Takagi T, Yoshida J. En bloc laminoplasty performed with threadwire saw. Neurosurgery. 2001; 48:235–239. PMID: 11152356.4. Hida S, Naito M, Arimizu J, Morishita Y, Nakamura A. The transverse placement laminoplasty using titanium miniplates for the reconstruction of the laminae in thoracic and lumbar lesion. Eur Spine J. 2006; 15:1292–1297. PMID: 16612643.
Article5. Iida Y, Kataoka O, Sho T, Sumi M, Hirose T, Bessho Y, et al. Postoperative lumbar spinal instability occurring or progressing secondary to laminectomy. Spine (Phila Pa 1976). 1990; 15:1186–1189. PMID: 2148439.
Article6. Kawahara N, Tomita K, Shinya Y, Matsumoto T, Baba H, Fujita T, et al. Recapping T-saw laminoplasty for spinal cord tumors. Spine (Phila Pa 1976). 1999; 24:1363–1370. PMID: 10404580.
Article7. Love JG. Laminectomy for the removal of spinal cord tumors. J Neurosurg. 1966; 25:116–121. PMID: 5947046.
Article8. Tredway TL, Santiago P, Hrubes MR, Song JK, Christie SD, Fessler RG. Minimally invasive resection of intradural-extramedullary spinal neoplasms. Neurosurgery. 2006; 58(1 Suppl):ONS52–ONS58. discussion ONS52-ONS58PMID: 16479629.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Restoration of the Spinous Process Following Muscle-Preserving Posterior Lumbar Decompression via Sagittal Splitting of the Spinous Process
- Extradural-Intradural Approach to Carotid-Ophthalmic Artery Aneurysm
- A Case Report of Intradural Ruptured Lumbar Disc
- Comparison of Spinous Process-Splitting Laminectomy versus Conventional Laminectomy for Lumbar Spinal Stenosis
- Twelve Contiguous Spinous Process Fracture of Cervico-Thoracic Spine
