Meningeal Layers Around Anterior Clinoid Process as a Delicate Area in Extradural Anterior Clinoidectomy : Anatomical and Clinical Study
- Affiliations
-
- 1Department of Neurosurgery, Eulji University Hospital, Daejeon, Korea. neurocsy@eulji.ac.kr
- 2Department of Neurosurgery, Mayo Clinic, Rochester, MN, USA.
- KMID: 2190658
- DOI: http://doi.org/10.3340/jkns.2012.52.4.391
Abstract
OBJECTIVE
Removal of the anterior clinoid process (ACP) is an essential process in the surgery of giant or complex aneurysms located near the proximal internal carotid artery or the distal basilar artery. An extradural clinoidectomy must be performed within the limits of the meningeal layers surrounding the ACP to prevent morbid complications. To identify the safest method of extradural exposure of the ACP, anatomical studies were done on cadaver heads.
METHODS
Anatomical dissections for extradural exposure of the ACP were performed on both sides of seven cadavers. Before dividing the frontotemporal dural fold (FTDF), we measured its length from the superomedial apex attached to the periorbita to the posterolateral apex which connects to the anterosuperior end of the cavernous sinus.
RESULTS
The average length of the FTDF on cadaver dissections was 7 mm on the right side and 7.14 mm on the left side. Cranial nerves were usually exposed when cutting FTDF more than 7 mm of the FTDF.
CONCLUSION
The most delicate area in an extradural anterior clinoidectomy is the junction of the FTDF and the anterior triangular apex of the cavernous sinus. The FTDF must be cut from the anterior side of the triangle at the periorbital side rather than from the dural side. The length of the FTDF incision must not exceed 7 mm to avoid cranial nerve injury.
Keyword
MeSH Terms
Figure
-
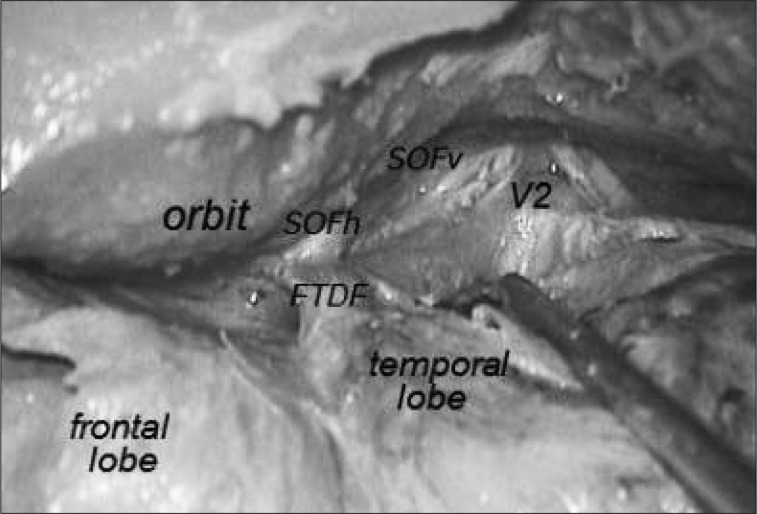
Fig. 1 Surgical anatomy of the right anterior clinoid process and surrounding neurovascular structures. SOFh : horizontal limb of the superior orbital fissure, SOFv : vertical limb of the superior orbital fissure, V2 : maxillary branch of the trigeminal nerve, FTDF : frontotemporal dural fold.
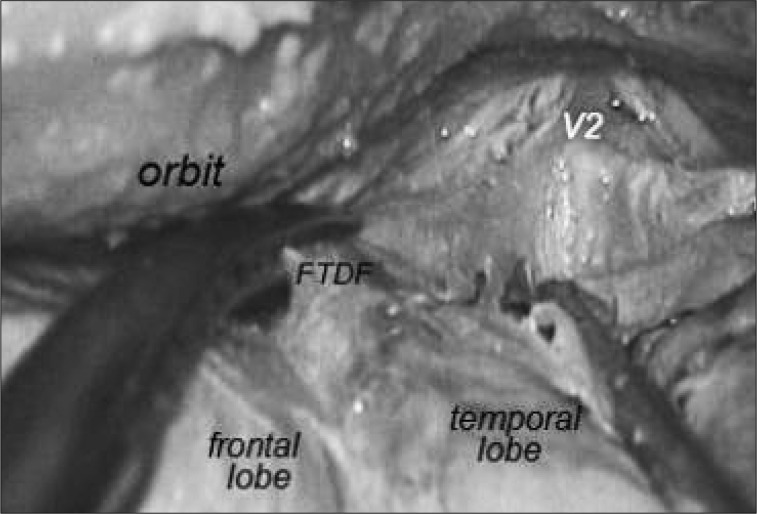
Fig. 2 To avoid injuring the cranial nerves, the horizontal meningeal limb of the superior orbital fissure must be cut in a direction parallel to the anterior clinoid process, not perpendicular to it, and from the anterior side of the triangle at the periorbital side rather than from the dural side. FTDF : frontotemporal dural fold, V2 : maxillary branch of trigeminal nerve.
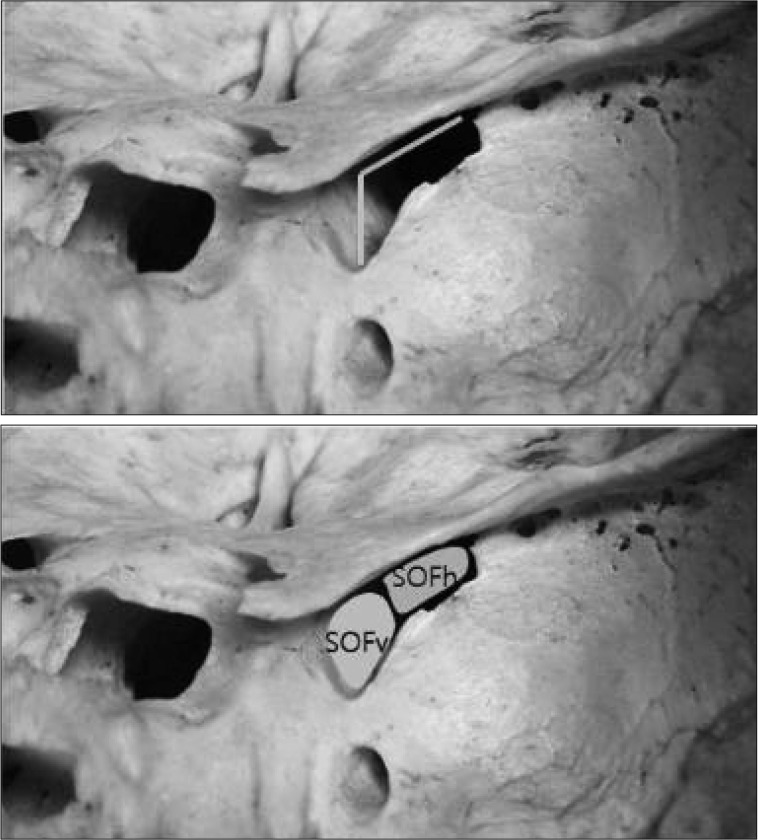
Fig. 3 Photographs showing the posterior view of the superior orbital fissure. The vertical neural limb (SOFv) and horizontal meningeal limb of the superior orbital fissure (SOFh) are schematically demonstrated.

Fig. 4 Photographs showing the relationship between the superior orbital fissure and neural structures on surgical position. The III, IV, V1 and V2 cranial nerves pass through the vertical neural limb of the superior orbital fissure (ellipse). The frontotemporal dural fold (FTDF) is within the horizontal meningeal limb of the superior orbital fissure (full line). The actual measurements are visible.
Reference
-
1. Avci E, Bademci G, Ozturk A. Microsurgical landmarks for safe removal of anterior clinoid process. Minim Invasive Neurosurg. 2005; 48:268–272. PMID: 16320187.
Article2. Bayassi S. [Meningo-orbital fold (MOF) as a guiding point in extradural approach to the anterior clinoid process]. Neurol Neurochir Pol. 2005; 39:49–55. PMID: 15735990.3. Collignon F, Link M. Paraclinoid and cavernous sinus regions : measurement of critical structures relevant for surgical procedure. Clin Anat. 2005; 18:3–9. PMID: 15597376.
Article4. Coscarella E, Başkaya MK, Morcos JJ. An alternative extradural exposure to the anterior clinoid process : the superior orbital fissure as a surgical corridor. Neurosurgery. 2003; 53:162–166. discussion 166-167. PMID: 12823885.5. Day AL. Aneurysms of the ophthalmic segment. A clinical and anatomical analysis. J Neurosurg. 1990; 72:677–691. PMID: 2324793.6. De Jesús O. The clinoidal space : anatomical review and surgical implications. Acta Neurochir (Wien). 1997; 139:361–365. PMID: 9202779.7. Dolenc VV. A combined epi- and subdural direct approach to carotid-ophthalmic artery aneurysms. J Neurosurg. 1985; 62:667–672. PMID: 3989589.
Article8. Dolenc VV. A combined transorbital-transclinoid and transsylvian approach to carotid-ophthalmic aneurysms without retraction of the brain. Acta Neurochir Suppl. 1999; 72:89–97. PMID: 10337416.
Article9. Dolenc VV. Carter LP, Spetzler RF, Hamilton MG, editors. Carotid-ophthalmic aneurysms. Neurovascular Surgery. 1994. New York: McGraw-Hill Inc;p. 673–686.10. Dolenc VV. Frontotemporal epidural approach to trigeminal neurinomas. Acta Neurochir (Wien). 1994; 130:55–65. PMID: 7725943.
Article11. Dolenc VV, Roger L. Microsurgical anatomy and surgery of the central skull base. 2003. Wien: Springer-Verlag.12. Froelich SC, Aziz KM, Levine NB, Theodosopoulos PV, van Loveren HR, Keller JT. Refinement of the extradural anterior clinoidectomy : surgical anatomy of the orbitotemporal periosteal fold. Neurosurgery. 2007; 61:179–185. discussion 185-186. PMID: 18091231.13. Gonzalez LF, Walker MT, Zabramski JM, Partovi S, Wallace RC, Spetzler RF. Distinction between paraclinoid and cavernous sinus aneurysms with computed tomographic angiography. Neurosurgery. 2003; 52:1131–1137. discussion 1138-1139. PMID: 12699558.
Article14. Inoue T, Rhoton AL Jr, Theele D, Barry ME. Surgical approaches to the cavernous sinus : a microsurgical study. Neurosurgery. 1990; 26:903–932. PMID: 2362670.15. Kawase T, van Loveren H, Keller JT, Tew JM. Meningeal architecture of the cavernous sinus : clinical and surgical implications. Neurosurgery. 1996; 39:527–534. discussion 534-536. PMID: 8875483.
Article16. Kim JM, Romano A, Sanan A, van Loveren HR, Keller JT. Microsurgical anatomic features and nomenclature of the paraclinoid region. Neurosurgery. 2000; 46:670–680. discussion 680-682. PMID: 10719864.
Article17. Mikami T, Minamida Y, Koyanagi I, Baba T, Houkin K. Anatomical variations in pneumatization of the anterior clinoid process. J Neurosurg. 2007; 106:170–174. PMID: 17236504.
Article18. Noguchi A, Balasingam V, Shiokawa Y, McMenomey SO, Delashaw JB Jr. Extradural anterior clinoidectomy. Technical note. J Neurosurg. 2005; 102:945–950. PMID: 15926728.19. Nutik SL. Removal of the anterior clinoid process for exposure of the proximal intracranial carotid artery. J Neurosurg. 1988; 69:529–534. PMID: 3418385.
Article20. Sade B, Kweon CY, Evans JJ, Lee JH. Enhanced exposure of carotico-oculomotor triangle following extradural anterior clinoidectomy : a comparative anatomical study. Skull Base. 2005; 15:157–161. discussion 161-162. PMID: 16175225.
Article21. Shi X, Han H, Zhao J, Zhou C. Microsurgical anatomy of the superior orbital fissure. Clin Anat. 2007; 20:362–366. PMID: 17080461.
Article22. Son HE, Park MS, Kim SM, Jung SS, Park KS, Chung SY. The avoidance of microsurgical complications in the extradural anterior clinoidectomy to paraclinoid aneurysms. J Korean Neurosurg Soc. 2010; 48:199–206. PMID: 21082045.
Article23. Yasargil MG, Gasser JC, Hodosh RM, Rankin TV. Carotid-ophthalmic aneurysms : direct microsurgical approach. Surg Neurol. 1977; 8:155–165. PMID: 897986.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Measurement of Critical Structures around Paraclinoidal Area : A Cadaveric Morphometric Study
- Anterior clinoid process and optic strut in Koreans
- Endoscopic Treatment of Anterior Clinoid Process Mucocele: 3 Cases
- The Avoidance of Microsurgical Complications in the Extradural Anterior Clinoidectomy to Paraclinoid Aneurysms
- The Pterional Approach and Extradural Anterior Clinoidectomy to Clip Paraclinoid Aneurysms
