Use of the pedicled buccal fat pad in the reconstruction of intraoral defects: a report of five cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Gangnam Severance Dental Hospital, College of Dentistry, Yonsei University, Seoul, Korea.
- 2Department of Oral and Maxillofacial Surgery, College of Dentistry, Yonsei University, Seoul, Korea. omsnam@yuhs.ac
- 3Department of Oral and Maxillofacial Surgery, Daejeon Dental Hospital, College of Dentistry, Wonkwang University, Daejeon, Korea.
- KMID: 2189710
- DOI: http://doi.org/10.5125/jkaoms.2012.38.2.116
Abstract
- The buccal fat pad is specialized fat tissue located anterior to the masseter muscle and deep to the buccinator muscle. Possessing a central body and four processes it provides separation allowing gliding motion between muscles, protects the neurovascular bundles from injuries, and maintains facial convexity. Because of its many advantageous functions, the use of the buccal fat pad during oral and maxillofacial procedures is promoted for the reconstruction of defects secondary to tumor resection, and those defects resulting from oroantral fistula caused by dento-alveolar surgery or trauma. We used the pedicled buccal fat pad in the reconstruction of intraoral defects such as oroantral fistula, maxillary posterior bone loss, or defects resulting from tumor resection. Epithelization of the fat tissue began 1 week after the surgery and demonstrated stable healing without complications over a long-term period. Thus, we highly recommend the use of this procedure.
Figure
-
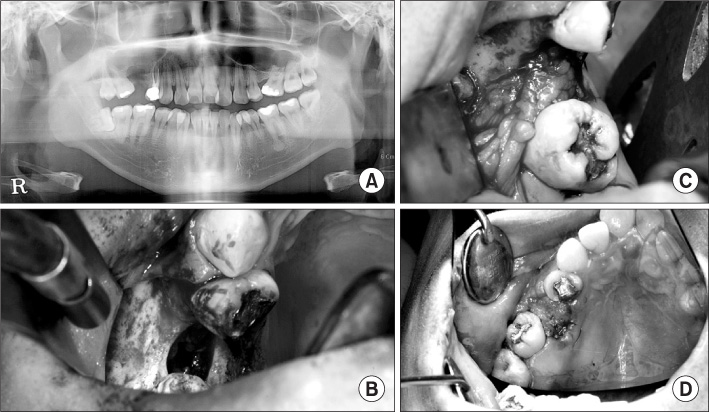
Fig. 1 Case 1. A. Preoperative dental panoramic X-ray. B. Intraoral view of oroantral fistula. C. Closed the oroantral fistula with buccal fat pad (size: 1×1 cm). D. One week after the operation. There was no bleeding and dehiscence.
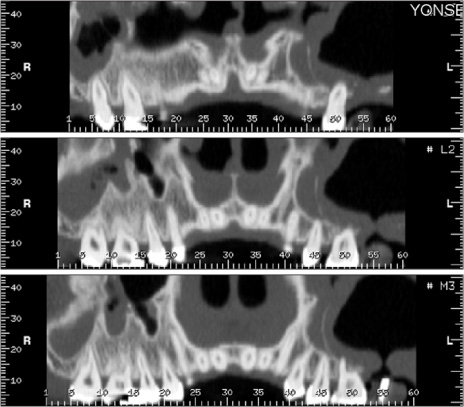
Fig. 2 Preoperative dental computed tomography image of case 2. Oroantral fistula was detected in the #27 area.

Fig. 3 Case 2. Primary closure with buccal fat pad measuring 1.5×1 cm (photographed using dental mirror).

Fig. 4 Preoperative computed tomography image of case 3 (horizontal view). Sequestrum was detected around the #25 root area.

Fig. 5 Case 3. A. Primary closure with buccal fat pad after the extraction of #25 and sequestrectomy of that area (size: 2.5×2 cm). B. One week after the operation.
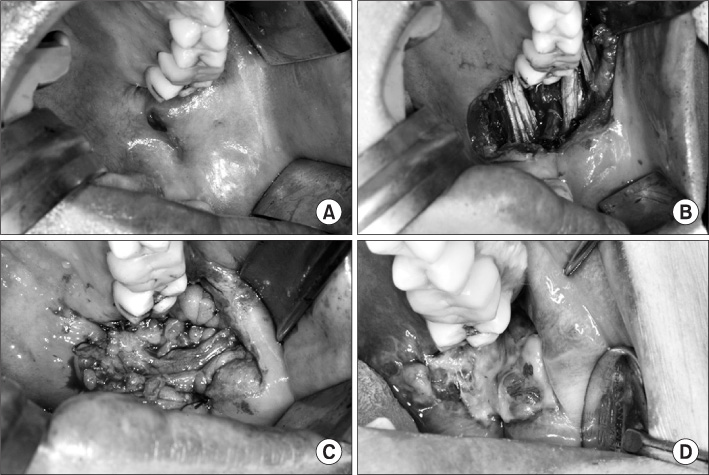
Fig. 6 Case 4. A. Reddish lesion on the posterior left buccal cheek area. B. Intraoral view after the resected tumor. C. Reconstruction with buccal fat pad after tumor resection. D. One week after operation (superficial necrosis was detected, but there was no dehiscence and bleeding).

Fig. 7 Case 5. A. Reconstruction of the posterior maxilla with buccal fat pad. B. One week after the operation. C. Three months after the operation. Epithelization was secured completely.
Cited by 1 articles
-
Reconstruction of partial maxillectomy defect with a buccal fat pad flap and application of 4-hexylresorcinol: a case report
Hyun Seok, Min-Keun Kim, Seong-Gon Kim
J Korean Assoc Oral Maxillofac Surg. 2016;42(6):370-374. doi: 10.5125/jkaoms.2016.42.6.370.
Reference
-
1. Egyedi P. Utilization of the buccal fat pad for closure of oroantral and/or oro-nasal communications. J Maxillofac Surg. 1977. 5:241–244.
Article2. Neder A. Use of buccal fat pad for grafts. Oral Surg Oral Med Oral Pathol. 1983. 55:349–350.
Article3. Tideman H, Bosanquet A, Scott J. Use of the buccal fat pad as a pedicled graft. J Oral Maxillofac Surg. 1986. 44:435–440.
Article4. Luskin IR. Reconstruction of oral defects using mucogingival pedicle flaps. Clin Tech Small Anim Pract. 2000. 15:251–259.
Article5. Alkan A, Dolanmaz D, Uzun E, Erdem E. The reconstruction of oral defects with buccal fat pad. Swiss Med Wkly. 2003. 133:465–470.6. Colella G, Tartaro G, Giudice A. The buccal fat pad in oral reconstruction. Br J Plast Surg. 2004. 57:326–329.
Article7. Baumann A, Ewers R. Application of the buccal fat pad in oral reconstruction. J Oral Maxillofac Surg. 2000. 58:389–392.
Article8. Amin MA, Bailey BM, Swinson B, Witherow H. Use of the buccal fat pad in the reconstruction and prosthetic rehabilitation of oncological maxillary defects. Br J Oral Maxillofac Surg. 2005. 43:148–154.
Article9. Hanazawa Y, Itoh K, Mabashi T, Sato K. Closure of oroantral communications using a pedicled buccal fat pad graft. J Oral Maxillofac Surg. 1995. 53:771–775.
Article10. Rapidis AD, Alexandridis CA, Eleftheriadis E, Angelopoulos AP. The use of the buccal fat pad for reconstruction of oral defects: review of the literature and report of 15 cases. J Oral Maxillofac Surg. 2000. 58:158–163.
Article11. Samman N, Cheung LK, Tideman H. The buccal fat pad in oral reconstruction. Int J Oral Maxillofac Surg. 1993. 22:2–6.
Article12. Singh J, Prasad K, Lalitha RM, Ranganath K. Buccal pad of fat and its applications in oral and maxillofacial surgery: a review of published literature (February) 2004 to (July) 2009. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010. 110:698–705.
Article13. Stuzin JM, Wagstrom L, Kawamoto HK, Baker TJ, Wolfe SA. The anatomy and clinical applications of the buccal fat pad. Plast Reconstr Surg. 1990. 85:29–37.
Article14. Zhang HM, Yan YP, Qi KM, Wang JQ, Liu ZF. Anatomical structure of the buccal fat pad and its clinical adaptations. Plast Reconstr Surg. 2002. 109:2509–2518.
Article15. Hao SP. Reconstruction of oral defects with the pedicled buccal fat pad flap. Otolaryngol Head Neck Surg. 2000. 122:863–867.
Article16. Poeschl PW, Baumann A, Russmueller G, Poeschl E, Klug C, Ewers R. Closure of oroantral communications with Bichat's buccal fat pad. J Oral Maxillofac Surg. 2009. 67:1460–1466.
Article17. Fujimura N, Nagura H, Enomoto S. Grafting of the buccal fat pad into palatal defects. J Craniomaxillofac Surg. 1990. 18:219–222.
Article18. Kim ES. Clinical evaluation of the effectiveness of pedicled buccal fat pad grafts in closure of oroantral communications. J Korean Assoc Oral Maxillofac Surg. 2000. 26:297–300.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The use of a pedicled buccal fat pad for reconstruction of posterior mandibular defects
- The use of buccal fat pad as a pedicled graft for the reconstruction of oral mucosal defect
- Reconstruction of large oroantral defects using a pedicled buccal fat pad
- Clinical Evaluation of the effectiveness of pedicled buccal fat pad grafts in closure of oroantral communications
- Clinical Experience of Buccal Fat Pad Pedicled Flap for Denuded Area in Palatoplasty
