Evaluation of the course of the inferior alveolar canal in the mandibular ramus using cone beam computed tomography
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Wonkwang University, Wonkwang Dental Research Institute, Iksan, Korea. kkhoms@daum.net
- KMID: 2189630
- DOI: http://doi.org/10.5125/jkaoms.2012.38.4.231
Abstract
OBJECTIVES
This study sought to provide guidelines in order to decrease the incidence of nerve injury during mandibular ramus bone harvesting, and to improve understanding of the anatomical structure of the inferior alveolar canal (IAC) to include its distance from the exterior buccal cortex.
MATERIALS AND METHODS
In January and February 2009, 20 patients who visited the Wonkwang University Department of Oral and Maxillofacial Surgery reporting various conditions underwent cone beam computed tomography and were included in this study. Patients with missing left or right mandibular first molars or incisors, or who had jaw fracture or bone pathologies, were excluded. The reference point (R point) was defined as the point where the occlusal plane reached the anterior ramus of the mandible. The position of the IAC in relation to the R point, the buccal bone width (BW), the alveolar crest distance (ACD), the distance from the alveolar crest to the occlusal plane (COD), and the distance from the IAC to the sagittal plane (CS) were determined using proprietary image analysis software which produced cross-sectional coronal and axial images.
RESULTS
The distance medially from the R point to the IAC along the axial plane was 6.19+/-1.21 mm. The HD from the R point, posteriorly to IAC, in the lateral view was 13.07+/-2.45 mm, the VD from the R point was 14.24+/-2.41 mm, and the ND from the R point was 10.12+/-1.76 mm. The pathway of the IAC was positioned almost in a straight line along a sagittal plane within 0.56+/-0.70 mm. The distance from the buccal bone surface to the IAC increased anteriorly from the R point.
CONCLUSION
Marking osteotomy lines in the retromolar area in procedures involving bone harvesting should be discouraged due to the risk of damage to IAC structures. Our measurements indicated that the area from the R point in the ramus of the mandible to 10 mm anterior can be safely harvested for bone grafting purposes.
MeSH Terms
Figure
-
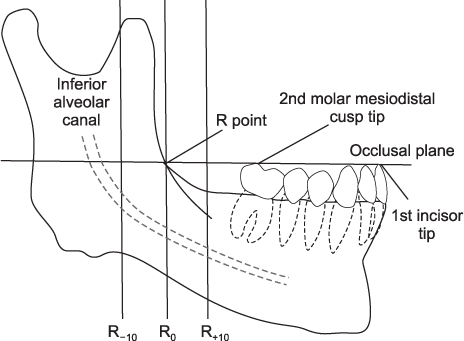
Fig. 1 Schematic of the mandible in lateral view. (R point: reference point)
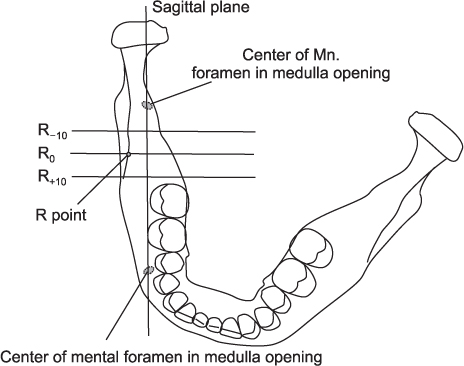
Fig. 2 Schematic of the mandible in superior view. (Mn.: mandible, R point: reference point)
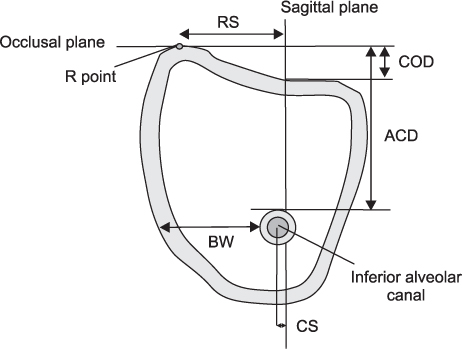
Fig. 3 Inferior alveolar canal, coronal cross-sectional. (R point: reference point, RS: R point to sagittal plane distance, COD: distance from the alveolar crest to the occlusal plane, ACD: alveolar crest distance, BW: buccal bone width, CS: distance from the inferior alveolar canal to the sagittal plane)
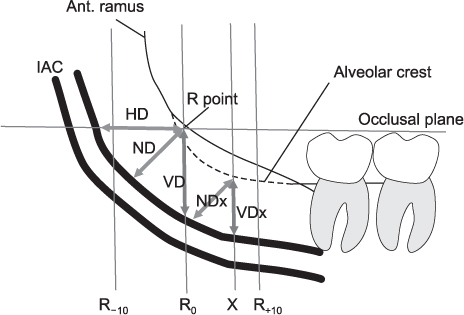
Fig. 4 Schematic of lateral view of IAC position measurements. (Ant.: anterior, IAC: inferior alveolar canal, R point: reference point, HD: horizontal distance, ND: nearest distance, VD: vertical distance, NDx: nearest distance on x plane, VDx: vertical distance on x plane, X: distance from baseline)
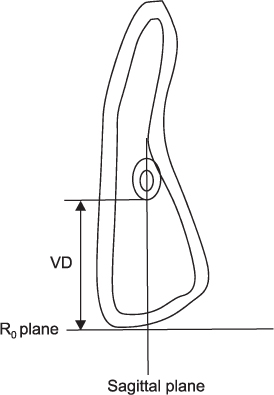
Fig. 5 IAC position measurements, cross-sectional occlusal plane. (IAC: inferior alveolar canal, VD: vertical distance, R: reference)
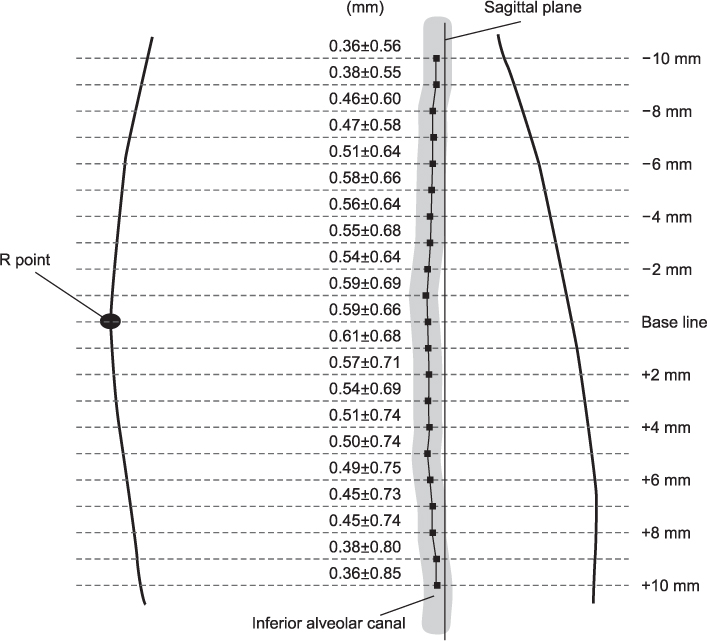
Fig. 6 Course of inferior alveolar canal along a sagittal plane (mean±standard deviation) (+10 mm=anterior, R point=buccal/lateral). (R point: reference point)
Cited by 1 articles
-
Prognosis in case of nerve disturbance after mandibular implant surgery in relation to computed tomography findings and symptoms
Ji Yeon Na, Sang-Sun Han, KugJin Jeon, Yoon Joo Choi, Seong Ho Choi, Chena Lee
J Periodontal Implant Sci. 2019;49(2):127-135. doi: 10.5051/jpis.2019.49.2.127.
Reference
-
1. Triplett RG, Schow SR. Autologous bone grafts and endosseous implants: complementary techniques. J Oral Maxillofac Surg. 1996. 54:486–494.
Article2. Jensen J, Sindet-Pedersen S, Oliver AJ. Varying treatment strategies for reconstruction of maxillary atrophy with implants: results in 98 patients. J Oral Maxillofac Surg. 1994. 52:210–216.
Article3. Habets LL, Bras J, Borgmeyer-Hoelen AM. Mandibular atrophy and metabolic bone loss. Endocrinology, radiology and histomorphometry. Int J Oral Maxillofac Surg. 1988. 17:208–211.4. Misch CE, Dietsh F. Bone-grafting materials in implant dentistry. Implant Dent. 1993. 2:158–167.
Article5. Silva FM, Cortez AL, Moreira RW, Mazzonetto R. Complications of intraoral donor site for bone grafting prior to implant placement. Implant Dent. 2006. 15:420–426.
Article6. Gowgiel JM. The position and course of the mandibular canal. J Oral Implantol. 1992. 18:383–385.7. Li N, Zhao B, Tan C. Intramandibular course and anatomic structure of the inferior alveolar nerve canal. Zhonghua Kou Qiang Yi Xue Za Zhi. 2001. 36:446–447.8. Kamburoglu K, Kilic C, Ozen T, Yuksel SP. Measurements of mandibular canal region obtained by cone-beam computed tomography: a cadaveric study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009. 107:e34–e42.9. Parikh SN. Bone graft substitutes: past, present, future. J Postgrad Med. 2002. 48:142–148.10. von Arx T, Kurt B. Implant placement and simultaneous peri-implant bone grafting using a micro titanium mesh for graft stabilization. Int J Periodontics Restorative Dent. 1998. 18:117–127.11. Yamamoto R, Nakamura A, Ohno K, Michi KI. Relationship of the mandibular canal to the lateral cortex of the mandibular ramus as a factor in the development of neurosensory disturbance after bilateral sagittal split osteotomy. J Oral Maxillofac Surg. 2002. 60:490–495.
Article12. Reich RH. Anatomical studies on the course of the mandibular canal. Dtsch Zahnarztl Z. 1980. 35:972–975.13. Levine MH, Goddard AL, Dodson TB. Inferior alveolar nerve canal position: a clinical and radiographic study. J Oral Maxillofac Surg. 2007. 65:470–474.
Article14. Ha SY, Song NK, Koh KJ. A computerized tomographic study on the location of the mandibular canal and the cortical thickness of the mandible. J Korean Acad Oral Maxillofac Radiol. 1997. 27:217–230.15. Misch CM. Comparison of intraoral donor sites for onlay grafting prior to implant placement. Int J Oral Maxillofac Implants. 1997. 12:767–776.16. Nkenke E, Radespiel-Troger M, Wiltfang J, Schultze-Mosgau S, Winkler G, Neukam FW. Morbidity of harvesting of retromolar bone grafts: a prospective study. Clin Oral Implants Res. 2002. 13:514–521.
Article17. Smith BR, Rajchel JL, Waite DE, Read L. Mandibular anatomy as it relates to rigid fixation of the sagittal ramus split osteotomy. J Oral Maxillofac Surg. 1991. 49:222–226.
Article18. Lavelle CL. Preliminary study of mandibular shape after tooth loss. J Prosthet Dent. 1985. 53:726–730.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of the relationship between the mandibular third molar and the mandibular canal using panoramic radiograph and cone beam computed tomography
- Radiographic evaluation of the course and visibility of the mandibular canal
- Anatomical position of the mandibular canal in relation to the buccal cortical bone: relevance to sagittal split osteotomy
- Sex determination by radiographic localization of the inferior alveolar canal using cone-beam computed tomography in an Egyptian population
- Diversion of the mandibular canal: Is it the best predictor of inferior alveolar nerve damage during mandibular third molar surgery on panoramic radiographs?
