Delayed Diagnosis of Acute Hematogenous Osteomyelitis of the Acetabulum: Report of Two Cases
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Soonchunhyang University, Cheonan, Korea. awe@korea.com
- KMID: 2186391
- DOI: http://doi.org/10.4055/jkoa.2009.44.1.145
Abstract
- Acute hematogenous osteomyelitis of the acetabulum is not a common disease with similar clinical symptoms and hematological findings to those of pyogenic arthritis of the hip joint. This symptom similarity might lead to a delayed diagnosis of the disease, and even to unnecessary surgery. We report two cases of acute hematogenous osteomyelitis of the acetabulum. One was a 13-year-old boy with non-specific radiological findings of the hip joint, who was initially diagnosed with fever of unknown origin. The other was an 11-year-old boy with hip joint pain and a recent history of minor trauma, which lead to a delayed diagnosis.
Keyword
MeSH Terms
Figure
-
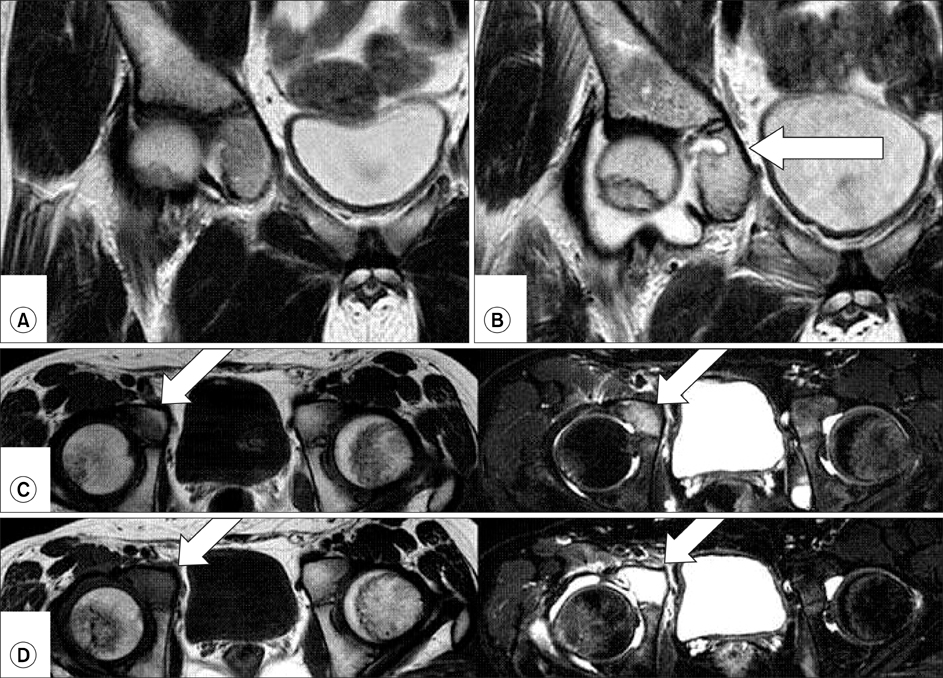
Fig. 1 (A) T2 weighted magnetic resonance imaging of a 13-year-old boy (case 1) with pain in the right hip was normal. (B) T2 weighted magnetic resonance imaging, taken when the symptoms relapsed, shows an abscess pocket (arrow) at the acetabulum near the triradiate cartilage. Fluid collection is shown in the hip joint. (C) The middle two images are of the initial magnetic resonance images. At the pubic portion of the acetabulum (arrow), the signal intensity of the right side was low in T1 weighted image, and high in T2-weighted image compared to that of the left side. (D) The bottom two images were taken when the symptoms relapsed. The difference on T1 weighted image and T2 weighted image are definite. There was fluid collection in the right hip joint.
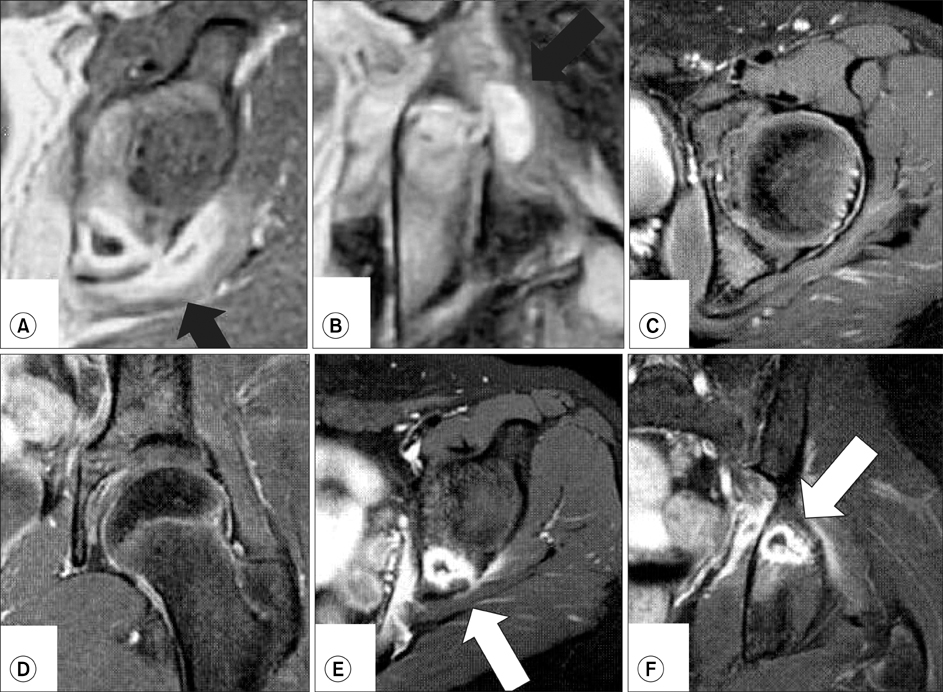
Fig. 2 A boy (case 2) age 11-year-old presented with a left hip joint pain and a recent minor trauma history. The abscess pocket with well-enhanced margins and cortical bone defect were shown on the T1 weighted axial (A) and coronal (B) magnetic resonance imaging taken from another hospital. The abscess had extended to the surrounding soft tissues (black arrow). On T2 weighted fat suppression axial (C) and coronal (D) magnetic resonance imaging, there was no fluid collection in the left hip joint and no specific findings were shown. On T2 weighted fat suppression axial (E) and coronal (F) magnetic resonance imaging taken after relapse, the abscess pocket with well-enhanced margins (white arrow) was still shown in the posterosuperior portion of the acetabulum.
Reference
-
1. Davidson D, Letts M, Khoshhal K. Pelvic osteomyelitis in children: a comparison of decades from 1980-1989 with 1990-2001. J Pediatr Orthop. 2003. 23:514–521.2. De Boeck H, Haentjens P, Verhaven E. Osteomyelitis of the actabulum. Acta Orthop Belg. 1990. 56:621–623.3. Edwards MS, Baker CJ, Granberry WM, Barrett FF. Pelvic osteomyelitis in children. Pediatrics. 1978. 61:62–67.4. Gamble JG, Rinsky LA, Bleck EE. Acetabular osteomyelitis in children. Clin Orthop Relat Res. 1984. 186:71–74.5. Highland TR, LaMont RL. Osteomyelitis of the pelvis in children. J Bone Joint Surg Am. 1983. 65:230–234.6. Klein JD, Leach KA. Pediatric pelvic osteomyelitis. Clin Pediatr (Phila). 2007. 46:787–790.7. Rand N, Mosheiff R, Matan Y, Porat S, Shapiro M, Liebergall M. Osteomyelitis of the pelvis. J Bone Joint Surg Br. 1993. 75:731–733.8. Suk SI, Lee CK, Ahn JK, et al. Orthopaedics. 2006. 6th ed. Seoul: Newest medical publishing company;272–274.9. Weber-Chrysochoou C, Corti N, Goetschel P, Altermatt S, Huisman TA, Berger C. Pelvic osteomyelitis: a diagnostic challenge in children. J Pediatr Surg. 2007. 42:553–557.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Observation of Hematogenous Osteomyelitis of Fibula in Children
- Diagnosis of Osteomyelitis by the Sequential Use of â¹â¹mTc - Methylene Diphosphonate and â¶â·Ga Imaging
- Hematogenous Osteomyelitis Occurred in Adult Long Bones
- Clinical Observation of Acute Hematogenous Osteomyelitis in Children
- A Clinical Study on Hematogenous Osteomyelitis in Children
