J Korean Med Assoc.
2006 Dec;49(12):1068-1081. 10.5124/jkma.2006.49.12.1068.
Bone Tumors Specific in Children
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonnam National University College of Medicine, Korea. stjung@chonnam.ac.kr, hikcj2005@naver.com
- KMID: 2184737
- DOI: http://doi.org/10.5124/jkma.2006.49.12.1068
Abstract
- Primary bone tumors in pediatric age group are uncommon, and even when they do occur, they are usually benign. The primary malignant tumors that occur predominantly in children are two bone tumors, namely, osteosarcoma and Ewing's sarcoma. An adequate history and physical examination are the first and most important steps in evaluating a patient with a bone tumor. All suspected bone tumors should be evaluated initially with plain roentgenograms. Then the additional diagnostic studies, such as computed tomography(CT), magnetic resonance imaging(MRI) and technetium bone scan can be used, if necessary. Biopsy should be the last step in evaluation. Most of benign bone tumors usually do not require treatment other than a periodic follow-up evaluation. The optimal treatment of the malignant bone tumor often requires a combination of radiation therapy, chemotherapy, and wide surgical excision or amputation. Early detection of a malignant bone tumor not only may make the difference between life and death but also may allow successful salvage surgery rather than amputation of the limb.
Keyword
MeSH Terms
Figure
-
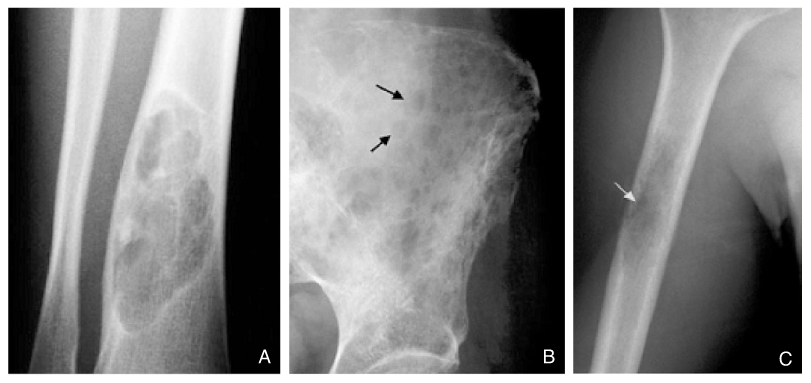
Figure 1 Different patterns of bone destruction
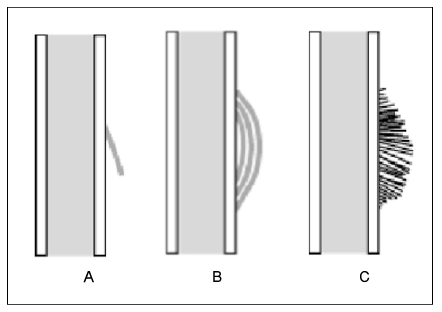
Figure 2 Different patterns of periosteal reaction
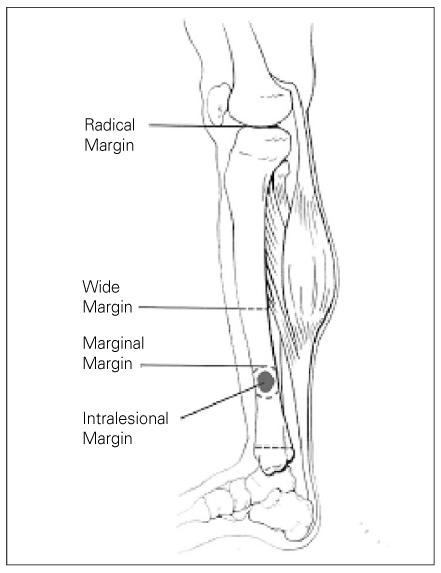
Figure 3 Surgical margins

Figure 4 Osteoid soteoma(CT)
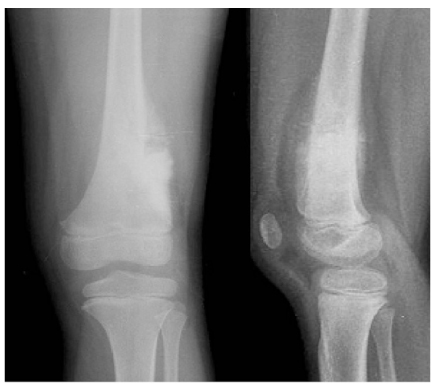
Figure 5 Conventional osteosarcoma

Figure 6 Conventional osteosarcoma

Figure 7 Osteochondroma
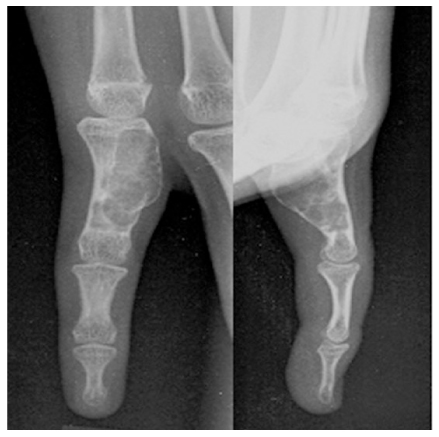
Figure 8 Enchondroma

Figure 9 Nonossifying fibroma

Figure 10 Shepherd's crook deformity of right hip
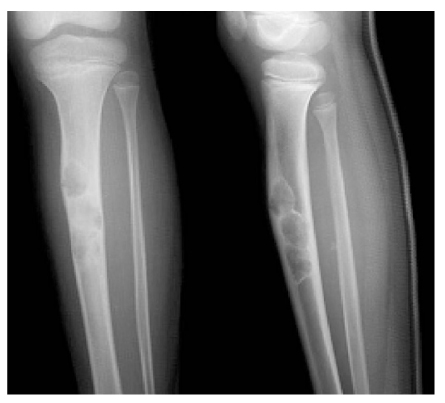
Figure 11 Osteofibrous dysplasia

Figure 12 Simple bone cyst

Figure 13 Ewing's sarcoma
Reference
-
1. Enneking W. Musculoskeletal tumor surgery. 1983. New York: Churchill Livingstone.2. Madwell JE, Ragsdale BD, Sweet DE. Radiologic and pathologic analysis of solitary bone lesions: Part I-Internal margins. Radiol Clin North Am. 1981. 19:715–748.3. Ragsdale BD, Madewell JE, Sweet DE. Radilogic and pathologic analysis of solitary bone lesions: Part II-periosteal reactions. Radiol Clin North Am. 1981. 19:749–783.4. Springfield DS, Gebghardt MC. Morrissy RT, Weinstein SL, editors. Bone and soft tissue tumors. Lovell and Winter's Pediatric Orthopaedics. 2001. 5th edition. Philadelphia: Lippincott Williams & Willinkins;507–562.5. Heinrich SD, Scarborough MT, editors. Pediatric Orthopaedic Oncology. Orthop Clin North Am. 1996.6. Jaramillo D, Laor T, Gebhardt MC. Pediatric musculoskeletal neoplasms: evaluation with MR imaging. Magn Reson Imaging Clin N Am. 1996. 4:749–770.7. Mankin HJ, Lange TA, Spanier S. The hazards of the biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg Am. 1982. 64:1121–1127.
Article8. Mankin Hj, Mankin CJ, Simon MA. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am. 1996. 78:656–663.9. Simon MA, Biermann JS. Biopsy of bone and soft-tissue lesions. J Bone Joint Surg Am. 1993. 75:616–621.
Article10. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980. 153:106–120.
Article11. Huvos AG. Bon tumors: Diagnosis, Treatment, and Prognosis. 1991. 2nd ed. Philadelphia: WB Saunders.12. Greenspan A, Remagen W. Differential Diagnosis of Tumors and Tumor like Lesions of Bone and Joints. 1998. Philadelphia: Lippincott-Raven.13. Himelstein BP, Dormans JP. Malignant bone tumors of childhood. Pediatr Clin North Am. 1996. 43:967–984.
Article14. Rougraff BT, Simon MA, Kneisl JS, Greenberg DB, Mankin HJ. Limb salvage compared with amputation for osteosarcoma of the distal end of the femur: a long-term ontological, functional, and quality-of-life study. J Bone Joint Surg Am. 1994. 76:649–656.
Article15. Copley L, Dormans JP. Benign pediatric bone tumors: Evaluation and treatment. Pediatr Clin North Am. 1996. 43:949–966.16. Dormans JP, Flynn JM. Beaty JH, Kasser JR, editors. Pathologic fracture associated with tumors and unique conditions of the muscoloskeletal edition. Rockwood and Wilkin's Fractures in Children. 2001. 5th ed. Philadelphia: Lippincott Williams & Wilkins.17. Dormans JP, Pill SG. Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect. 2002. 51:457–467.18. Grabias SL, Campbell CJ. Fibrous dysplasia. Orthop Clin North Am. 1977. 8:771–783.
Article19. Martinez V, Sissons HA. Aneurysmal bone cyst: a review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer. 1988. 61:2291–2304.
Article20. Szendroi M, Arato G, Ezzati A, Huttl K, Szavcsur P. Aneurysmal bone cyst: its pathogenesis based on angiographic, immunohistochemical and eletron microscopic studies. Pathol Oncol Res. 1998. 4:277–281.21. Dormans JP, Hanna BG, Johnston DR, Khurana JS. Surgical treatment and recurrence rate of aneurysmal bone cysts in children. Clin Orthop. 2004. 421:205–211.
Article22. Sessa S, Sommelet D, Lascombes P, Prevot J. Treatment of Langerhans-cell histiocytosis in children: experience at the Children's hospital of Nancy. J Bone Joint Surg Am. 1994. 76:1513–1525.
Article23. Bernstrand C, Bjork O, Ahstrom L, Henter JI. Intralesional steroids in Langerhans cell histiocytosis of bone. Acta Paediatr. 1996. 85:502–504.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Resection of Malignant Bone Tumors
- Growth Expectation in Children: Leg Length Discrepancy Related with Bone Tumor in Children
- Malignancies in children who present with bone pain
- Bone modeling, remodeling, and skeletal health in children and adolescents: mineral accrual, assessment and treatment
- Giant Cell Tumor of Short Tubular Bone: Case Report
