A Case of an Anomalous Hypertrophied Muscle Band in the Left Ventricle
- Affiliations
-
- 1Department of Internal Medicine, Gumi Gang Dong Hospital, Gumi, Korea.
- 2Division of Cardiology, Department of Internal Medicine, Kumi CHA Medical Center, CHA University College of Medicine, Gumi, Korea.
- 3Division of Cardiology, Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea. ddhyang@knu.ac.kr
- KMID: 2177373
- DOI: http://doi.org/10.4250/jcu.2012.20.2.97
Abstract
- A hypertrophied muscle band (HMB) in the left ventricle (LV), which can be misinterpreted as apical hypertrophic cardiomyopathy, is a rare echocardiographic finding in a patient with normal LV wall thickness. Not only are symptoms produced, but changes in the electrocardiogram (ECG) are limited to the repolarization phase and show no progression even in a large HMB. Hence, we report a case of a 25-year-old woman who visited a local medical clinic due to epigastric discomfort in January 2007. The 24-hour Holter ECG showed multiple premature ventricular complexes. An HMB (3.23 x 10.8 cm) was observed on two-dimensional echocardiography that ran toward the interventricular septum (IVS) across the LV and divided the LV into apical and basal cavities at the apical one-third of the LV. Although LV wall thickness showed normal range, flow acceleration was observed between the HMB and IVS and revealed dagger-shaped with a high pressure gradient up to 30 mmHg in continuous wave Doppler examination. Circumferential band-like myocardial hypertrophy was observed at the LV apex on cardiac magnetic resonance imaging. Myocardial thinning and prominent trabeculae were present from the proximal to distal HMB. However, contractility was normal at the myocardial thinning site, regional wall motion abnormality was not observed in cine images. Focal fatty accumulation was evident at the base of the HMB. Coronary angiography revealed no significant stenosis, whereas left ventriculography showed septation at the apical one-third of the LV. The patient was discharged without any medication.
Keyword
MeSH Terms
Figure
-

Fig. 1 Electrocardiogram showing multiple junctional complexes (arrows).

Fig. 2 Modified parasternal long-axis view showing the hypertrophied muscle band (arrow) that run toward the interventricular septum across the left ventricle (LV) and divide the LV into apical and basal cavities at its apical one-third region (A). Apical four-chamber view showing the hypertrophied muscle band (arrow) that run toward the interventricular septum, across the LV, and divide the LV into apical and basal cavities (B).

Fig. 3 Continuous wave Doppler examination showing flow acceleration between the hypertrophied muscle band and interventricular septum and dagger-shaped with a high pressure gradient up to 30 mmHg (arrows).
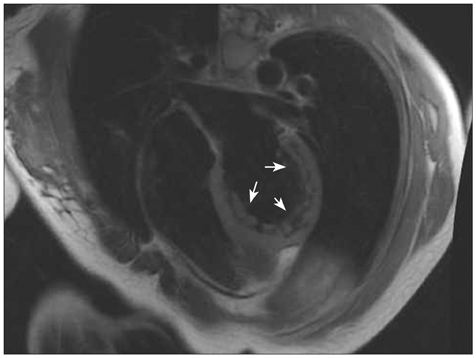
Fig. 4 Cardiac magnetic resonance image showing the circumferential band-like myocardial hypertrophy at the left ventricular apex (arrows).

Fig. 5 Left ventriculogram showing septation in the apical one-third of the left ventricle (arrows).
Reference
-
1. Salazar J. Left ventricular anomalous muscle band and electrocardiographic repolarization changes. Pediatr Cardiol. 1997. 18:434–436.
Article2. Sutton MG, Dubrey S, Oldershaw PJ. Muscular false tendons, aberrant left ventricular papillary musculature, and severe electrocardiographic repolarisation abnormalities: a new syndrome. Br Heart J. 1994. 71:187–190.
Article3. Maron BJ. Apical hypertrophic cardiomyopathy: the continuing saga. J Am Coll Cardiol. 1990. 15:91–93.
Article4. Sakamoto T, Tei C, Murayama M, Ichiyasu H, Hada Y. Giant T wave inversion as a manifestation of asymmetrical apical hypertrophy (AAH) of the left ventricle. Echocardiographic and ultrasono-cardiotomographic study. Jpn Heart J. 1976. 17:611–629.
Article5. Yamaguchi H, Ishimura T, Nishiyama S, Nagasaki F, Nakanishi S, Takatsu F, Nishijo T, Umeda T, Machii K. Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy): ventriculographic and echocardiographic features in 30 patients. Am J Cardiol. 1979. 44:401–412.
Article6. Tsunakawa H, Wei D, Mashima S, Harumi K. Study on the genesis of giant negative T wave in apical hypertrophic cardiomyopathy using a three-dimensional computer model. Jpn Heart J. 1991. 32:799–809.
Article7. Webb JG, Sasson Z, Rakowski H, Liu P, Wigle ED. Apical hypertrophic cardiomyopathy: clinical follow-up and diagnostic correlates. J Am Coll Cardiol. 1990. 15:83–90.
Article8. Kay PH, Rigby M, Mulholland HC. Congenital double chambered left ventricle treated by exclusion of accessory chamber. Br Heart J. 1983. 49:195–198.
Article9. Vaidiyanathan D, Prabhakar D, Selvam K, Alagesan R, Thirunavukarasu N, Muthukumar D. Isolated congenital left ventricular diverticulum in adults. Indian Heart J. 2001. 53:211–213.10. Rickli H, Attenhofer Jost CH, Locher JT, Jenni R. Double-chambered left ventricle: unusual presentation with an apical defect in a thallium scan in a middle-aged, asymptomatic woman. Echocardiography. 1999. 16:387–391.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anomalous Connection of Umbilical Vessels to the Left Ventricle: Case Report
- An Anatomical Description of the Anomalous Nasi Muscle
- Two Cases of Double-Chambered Right Ventricle without Other Congenital Cardiac Anomalies
- Left Ventricular Anomalous Muscle Band and Electrocardiographic Repolarization Changes in a 5 Year Old Girl
- Two-chambered right ventricle resulting from aberrant muscle bundles a case report
