Mechanical and biological complication rates of the modified lateral-screw-retained implant prosthesis in the posterior region: an alternative to the conventional Implant prosthetic system
- Affiliations
-
- 1Department of Periodontology, Research Institute for Periodontal Regeneration, College of Dentistry, Yonsei University, Seoul, Republic of Korea.
- 2Department of Periodontology, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea. youngtaek77@naver.com
- 3Department of Prosthodontics, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea.
- KMID: 2176658
- DOI: http://doi.org/10.4047/jap.2016.8.2.150
Abstract
- PURPOSE
The modified lateral-screw-retained implant prosthesis (LSP) is designed to combine the advantages of screw- and cement-retained implant prostheses. This retrospective study evaluated the mechanical and biological complication rates of implant-supported single crowns (ISSCs) inserted with the modified LSP in the posterior region, and determined how these complication rates are affected by clinical factors.
MATERIALS AND METHODS
Mechanical complications (i.e., lateral screw loosening [LSL], abutment screw loosening, lateral screw fracture, and ceramic fracture) and biological complications (i.e., peri-implant mucositis [PM] and peri-implantitis) were identified from the patients' treatment records, clinical photographs, periapical radiographs, panoramic radiographs, and clinical indices. The correlations between complication rates and the following clinical factors were determined: gender, age, position in the jaw, placement location, functional duration, clinical crown-to-implant length ratio, crown height space, and the use of a submerged or nonsubmerged placement procedure.
RESULTS
Mechanical and biological complications were present in 25 of 73 ISSCs with the modified LSP. LSL (n=11) and PM (n=11) were the most common complications. The incidence of mechanical complications was significantly related to gender (P=.018). The other clinical factors were not significantly associated with mechanical and biological complication rates.
CONCLUSION
Within the limitations of this study, the incidence of mechanical and biological complications in the posterior region was similar for both modified LSP and conventional implant prosthetic systems. In addition, the modified LSP is amenable to maintenance care, which facilitates the prevention and treatment of mechanical and biological complications.
Keyword
MeSH Terms
Figure
-
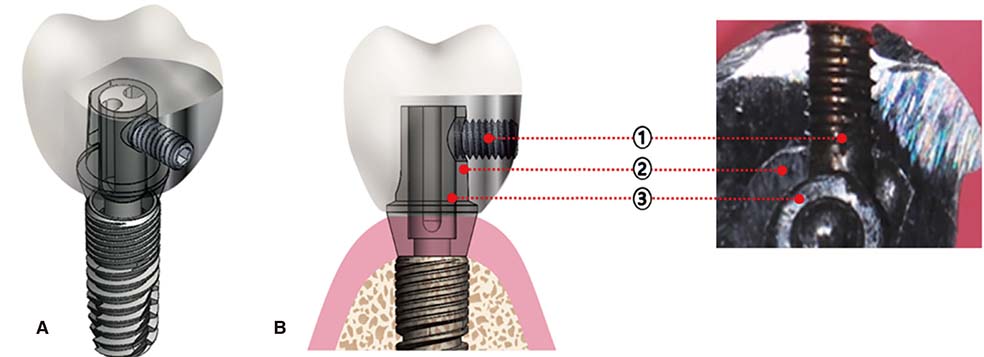
Fig. 1 Three-dimensional view (A), cross-sectional view and photograph (B) of the modified lateral-screw-retained implant prosthesis (LSP). The modified LSP consists of a lateral screw, an abutment with a lateral hole, an antiloosening abutment screw, and a crown with a negative screw housing (1, lateral [transverse] screw; 2, abutment; 3, abutment screw).
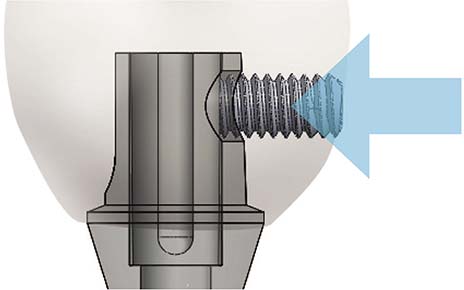
Fig. 2 The modified LSP retains the implant prosthesis by the application of a pushing force onto the abutment (arrow). This system has a negative screw housing located within the crown, which provides mechanical locking by pushing against the walls of the abutment. The lateral screw penetrates the abutment to make direct contact with the abutment screw.
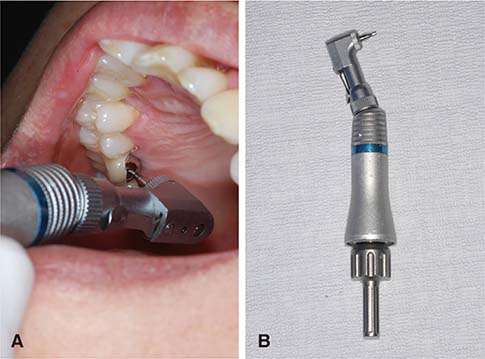
Fig. 3 (A) The modified LSP does not involve access-hole resin or sealing materials, and so the occurrence of lateral screw loosening (LSL) can be clinically verified by visually checking the lateral screw access hole. The lateral screw can be tightened if necessary using a lateral screwdriver with a contra-angle attachment. The implant abutment/crown is manually tightened to a torque of 5-10 Ncm. (B) Since the lateral screw is designed for use with a lateral screwdriver and a contra-angle attachment, it is easily managed within the oral cavity.
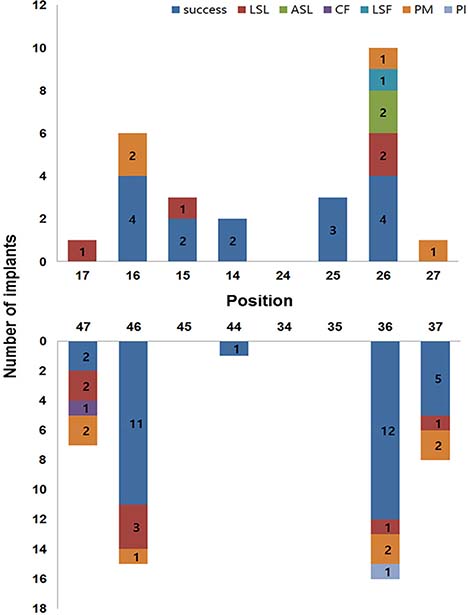
Fig. 4 Frequency distribution of implants according to their position in the jaw and the complication rates of the implant-supported single crowns (ISSCs) with the modified LSP in the posterior region. ASL, abutment screw loosening; LSF, lateral screw fracture; CF, ceramic fracture; PM, peri-implant mucositis; PI, peri-implantitis.

Fig. 5 Incidence of mechanical and biological complications according to the duration of functional loading.
Reference
-
1. Kotsovilis S, Fourmousis I, Karoussis IK, Bamia C. A systematic review and meta-analysis on the effect of implant length on the survival of rough-surface dental implants. J Periodontol. 2009; 80:1700–1718.2. Moraschini V, Velloso G, Luz D, Barboza EP. Implant survival rates, marginal bone level changes, and complications in full-mouth rehabilitation with flapless computer-guided surgery: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2015; 44:892–901.3. Wöhrle PS. Nobel Perfect esthetic scalloped implant: rationale for a new design. Clin Implant Dent Relat Res. 2003; 5:64–73.4. Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001; 72:1364–1371.5. Funato A, Salama MA, Ishikawa T, Garber DA, Salama H. Timing, positioning, and sequential staging in esthetic implant therapy: a four-dimensional perspective. Int J Periodontics Restorative Dent. 2007; 27:313–323.6. Weigl P. New prosthetic restorative features of Ankylos implant system. J Oral Implantol. 2004; 30:178–188.7. Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin Oral Implants Res. 2008; 19:119–130.8. Jung RE, Zembic A, Pjetursson BE, Zwahlen M, Thoma DS. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin Oral Implants Res. 2012; 23:2–21.9. Pjetursson BE, Brägger U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97–113.10. Hermanides L. Criteria to manage the technical and biologic success of an implant abutment. Compend Contin Educ Dent. 2014; 35:463–468.11. Pjetursson BE, Tan K, Lang NP, Brägger U, Egger M, Zwahlen M. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin Oral Implants Res. 2004; 15:667–676.12. Linkevicius T, Vladimirovas E, Grybauskas S, Puisys A, Rutkunas V. Veneer fracture in implant-supported metal-ceramic restorations. Part I: Overall success rate and impact of occlusal guidance. Stomatologija. 2008; 10:133–139.13. Karl M, Graef F, Wichmann MG, Heckmann SM. The effect of load cycling on metal ceramic screw-retained implant restorations with unrestored and restored screw access holes. J Prosthet Dent. 2008; 99:19–24.14. Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. Periodontol 2000. 1998; 17:63–76.15. Klinge B, Meyle J. Working Group 2. Peri-implant tissue destruction. The Third EAO Consensus Conference 2012. Clin Oral Implants Res. 2012; 23:108–110.16. Misch CE, Goodacre CJ, Finley JM, Misch CM, Marinbach M, Dabrowsky T, English CE, Kois JC, Cronin RJ Jr. Consensus conference panel report: crown-height space guidelines for implant dentistry-part 1. Implant Dent. 2005; 14:312–318.17. Blanes RJ, Bernard JP, Blanes ZM, Belser UC. A 10-year prospective study of ITI dental implants placed in the posterior region. I: Clinical and radiographic results. Clin Oral Implants Res. 2007; 18:699–706.18. Kreissl ME, Gerds T, Muche R, Heydecke G, Strub JR. Technical complications of implant-supported fixed partial dentures in partially edentulous cases after an average observation period of 5 years. Clin Oral Implants Res. 2007; 18:720–726.19. Theoharidou A, Petridis HP, Tzannas K, Garefis P. Abutment screw loosening in single-implant restorations: a systematic review. Int J Oral Maxillofac Implants. 2008; 23:681–690.20. Cha HS, Kim YS, Jeon JH, Lee JH. Cumulative survival rate and complication rates of single-tooth implant; focused on the coronal fracture of fixture in the internal connection implant. J Oral Rehabil. 2013; 40:595–602.21. Morneburg TR, Pröschel PA. In vivo forces on implants influenced by occlusal scheme and food consistency. Int J Prosthodont. 2003; 16:481–486.22. Simonis P, Dufour T, Tenenbaum H. Long-term implant survival and success: a 10-16-year follow-up of non-submerged dental implants. Clin Oral Implants Res. 2010; 21:772–777.23. Bidra AS. Nonsurgical management of inflammatory periimplant disease caused by food impaction: a clinical report. J Prosthet Dent. 2014; 111:96–100.24. Korsch M, Robra BP, Walther W. Predictors of excess cement and tissue response to fixed implant-supported dentures after cementation. Clin Implant Dent Relat Res. 2015; 17:e45–e53.25. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009; 80:1388–1392.26. Lindhe J, Meyle J. Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:282–285.27. Heitz-Mayfield LJ, Salvi GE, Botticelli D, Mombelli A, Faddy M, Lang NP. Implant Complication Research Group. Anti-infective treatment of peri-implant mucositis: a randomised controlled clinical trial. Clin Oral Implants Res. 2011; 22:237–241.28. Heitz-Mayfield LJ, Salvi GE, Mombelli A, Faddy M, Lang NP. Implant Complication Research Group. Anti-infective surgical therapy of peri-implantitis A 12-month prospective clinical study. Clin Oral Implants Res. 2012; 23:205–210.29. Abrahamsson I, Berglundh T, Lindhe J. The mucosal barrier following abutment dis/reconnection. An experimental study in dogs. J Clin Periodontol. 1997; 24:568–572.30. Biancu S, Ericsson I, Lindhe J. Periodontal ligament tissue reactions to trauma and gingival inflammation. An experimental study in the beagle dog. J Clin Periodontol. 1995; 22:772–779.31. Miyaura K, Matsuka Y, Morita M, Yamashita A, Watanabe T. Comparison of biting forces in different age and sex groups: a study of biting efficiency with mobile and non-mobile teeth. J Oral Rehabil. 1999; 26:223–227.32. Ferrario VF, Sforza C, Serrao G, Dellavia C, Tartaglia GM. Single tooth bite forces in healthy young adults. J Oral Rehabil. 2004; 31:18–22.33. Rangert BR, Sullivan RM, Jemt TM. Load factor control for implants in the posterior partially edentulous segment. Int J Oral Maxillofac Implants. 1997; 12:360–370.34. Nissan J, Ghelfan O, Gross O, Priel I, Gross M, Chaushu G. The effect of crown/implant ratio and crown height space on stress distribution in unsplinted implant supporting restorations. J Oral Maxillofac Surg. 2011; 69:1934–1939.35. Esposito M, Ekestubbe A, Gröndahl K. Radiological evaluation of marginal bone loss at tooth surfaces facing single Brånemark implants. Clin Oral Implants Res. 1993; 4:151–157.36. Tarnow D, Elian N, Fletcher P, Froum S, Magner A, Cho SC, Salama M, Salama H, Garber DA. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003; 74:1785–1788.37. Lee JH, Lee JB, Park JI, Choi SH, Kim YT. Mechanical complication rates and optimal horizontal distance of the most distally positioned implant-supported single crowns in the posterior region: a study with a mean follow-up of 3 years. J Prosthodont. 2015; 24:517–524.38. Cicciù M, Beretta M, Risitano G, Maiorana C. Cemented-retained vs screw-retained implant restorations: an investigation on 1939 dental implants. Minerva Stomatol. 2008; 57:167–179.39. Cicciu M, Bramanti E, Matacena G, Guglielmino E, Risitano G. FEM evaluation of cemented-retained versus screw-retained dental implant single-tooth crown prosthesis. Int J Clin Exp Med. 2014; 7:817–825.40. Dierens M, DeBruyn H, Kisch J, Nilner K, Cosyn J, Vandeweghe S. Prosthetic Survival and Complication Rate of Single Implant Treatment in the Periodontally Healthy Patient after 16 to 22 Years of Follow-Up. Clin Implant Dent Relat Res. 2014; 09. 05.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical cases of implant-supported fixed dental prosthesis using modified lingual screw system (T-screw system)
- Implant-Supported Fixed Dental Prostheses with New Retention Type Using Zirconia Ball and Nickel-Titanium Spring
- Clinical evaluation of retained preload and cement washout in screw- and cement-retained implant prosthesis
- Submucosal zirconia implant prosthesis fabricated with CAD/CAM
- Retrievable SCP (screw-cement prosthesis) implant-supported fixed partial dentures in a fully edentulous patient: a case report
