Solitary Small Bowel Metastasis from Breast Cancer
- Affiliations
-
- 1Department of Surgery, Yeungnam University College of Medicine, Daegu, Korea. crystallee@med.yu.ac.kr
- 2Department of Pathology, Yeungnam University College of Medicine, Daegu, Korea.
- 3Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea.
- KMID: 2175646
- DOI: http://doi.org/10.4048/jbc.2011.14.1.69
Abstract
- The common sites of metastasis of breast cancer are bone, lung, and liver, but gastrointestinal metastasis from breast cancer is rare. We experienced a case of solitary ileal metastasis from breast cancer. A 45-years-old woman presented with melena for several weeks. She showed no other abdominal symptoms. Colonoscopy findings showed an ulcerative mucosal lesion in the terminal ileum, and biopsy was performed. Pathologic examination revealed metastatic carcinoma, originated from breast. The tumor cells were positive for estrogen receptor and negative for Cdx-2. She had had a previous medical history of bilateral breast cancer and undergone breast conserving surgery with sentinel lymph node biopsy for both breasts. The torso positron emission tomography scan at 19 months after surgery showed mildly increased uptake in the terminal ileum which was considered as inflammation. Finally, she was diagnosed with solitary ileal metastasis from breast cancer at 22 months after surgery.
Keyword
MeSH Terms
Figure
-

Figure 1 Colonoscopy showed ulcerative mucosa (arrow) in the terminal ileum.
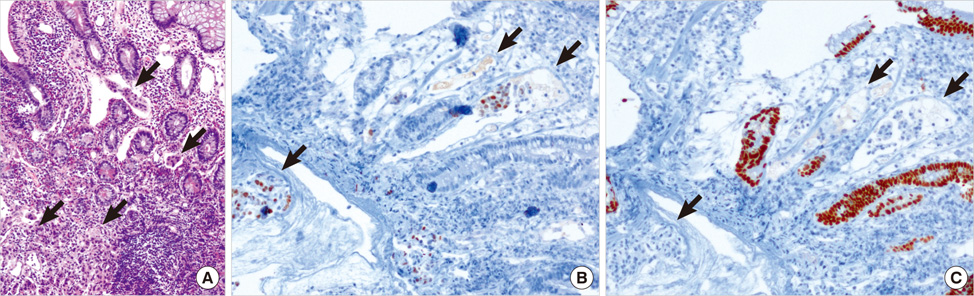
Figure 2 (A) Microscopic findings of terminal ileal wall showed tumor emboli infiltrations (arrows) in lamina propria lymphatic spaces, but intact mucosal epithelium (H&E stain, ×100). (B) The tumor cells (arrows) were positive for estrogen receptor; (C) negative for Cdx-2, a critical nuclear transcription factor for intestinal development (immunohistochemical staining, ×100).
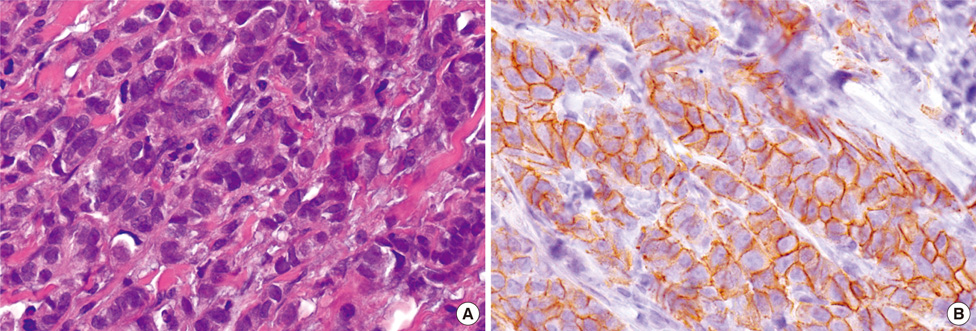
Figure 3 (A) Microscopic findings of both breast revealed infiltration of malignant ductal cells. The primary invasive ductal carcinomas of breast shows well differentiation and no lymphovascular invasions (H&E stain, ×200). (B) The malignant cells are positive for E-cadherin (immunohistochemical staining, ×200).
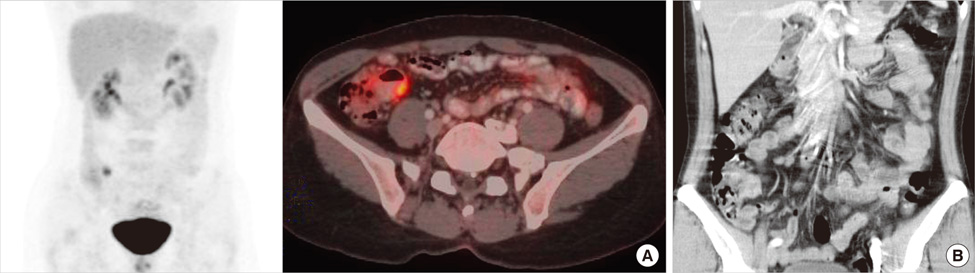
Figure 4 (A) The torso positron emission tomography scan showed mild uptake in the terminal ileum (SUV max=5.7). (B) The retroperitoneal computed tomography showed thickening of the wall of terminal ileum and multiple lymph node enlargement around them.
Cited by 3 articles
-
Small bowel obstruction from distant metastasis of primary breast cancer: a case report
Seung Jae Oh, Seon Young Park, Ji Young Kim, Hyunee Yim, Yongsik Jung, Sae Hwan Han
Ann Surg Treat Res. 2018;94(2):102-105. doi: 10.4174/astr.2018.94.2.102.Peritoneal and gastric metastasis from invasive lobular breast carcinoma: a case report
Yoon Seok Kim, Eun Ae Jae, Dong Won Ryu, Chung Han Lee
Kosin Med J. 2015;30(1):87-92. doi: 10.7180/kmj.2015.30.1.87.Small Bowel Metastatic Cancer Observed With Double Balloon Enteroscopy in a Patient With a Past History of Multiple Cancers
Ji Young Song, Beom Jae Lee, Eun Sang Yu, Young Ju Na, Jong-Jae Park, Jae Seon Kim, Young-Tae Bak
Intest Res. 2015;13(4):350-354. doi: 10.5217/ir.2015.13.4.350.
Reference
-
1. Harris JR. Diseases of the Breast. 2004. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;1101–1159.2. Oyasiji T, Shoemake P, Bakhos C, Mansourian V. Small bowel obstruction from metastatic breast cancer masquerading as an obstructed incisional hernia. Conn Med. 2009. 73:403–406.3. Braasch JW, Denbo HE. Tumors of the small intestine. Surg Clin North Am. 1964. 44:791–809.4. Borst MJ, Ingold JA. Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast. Surgery. 1993. 114:637–641.5. Nazareno J, Taves D, Preiksaitis HG. Metastatic breast cancer to the gastrointestinal tract: a case series and review of the literature. World J Gastroenterol. 2006. 12:6219–6224.
Article6. Hansen RM, Lewis JD, Janjan NA, Komorowski RA. Occult carcinoma of the breast masquerading as primary adenocarcinoma of the small intestine. A case report. J Clin Gastroenterol. 1988. 10:213–217.
Article7. Chang SF, Burrell MI, Brand MH, Garsten JJ. The protean gastrointestinal manifestations of metastatic breast carcinoma. Radiology. 1978. 126:611–617.
Article8. Schwarz RE, Klimstra DS, Turnbull AD. Metastatic breast cancer masquerading as gastrointestinal primary. Am J Gastroenterol. 1998. 93:111–114.
Article9. de la Monte SM, Hutchins GM, Moore GW. Estrogen and progesterone receptors in prediction of metastatic behavior of breast carcinoma. Am J Med. 1984. 76:11–17.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Small Bowel Metastasis from Breast Cancer: A Case Report
- Small bowel obstruction from distant metastasis of primary breast cancer: a case report
- Radiological and Histological Clues in the Diagnosis of Solitary and Synchronous Breast Metastasis From Small Cell Lung Carcinoma
- Localized Metastasis to Small and Large Bowel from Breast Cancer: A Case Report
- Two Cases of Cutaneous Metastasis from Small Cell Lung Cancer
