Assessment of Posterior Globe Flattening: Two-Dimensional versus Three-Dimensional T2-Weighted Imaging
- Affiliations
-
- 1Department of Radiology, Gachon University Gil Medical Center, Incheon, Korea. neuroradkim@gmail.com
- KMID: 2175612
- DOI: http://doi.org/10.13104/imri.2015.19.3.178
Abstract
- PURPOSE
To compare the frequency of posterior globe flattening between two-dimensional T2-weighted imaging (2D T2WI) and three-dimensional (3D T2WI).
MATERIALS AND METHODS
Sixty-nine patients (31 female; mean age, 44.4 years) who had undergone both 5-mm axial T2WI and sagittal 3D 1-mm isovoxel T2WI of the whole brain for evaluation of various diseases (headache [n = 30], large hemorrhage [n = 19], large tumor or leptomeningeal tumor spread [n = 15], large infarct [n = 3], and bacterial meningitis [n = 2]) were used in this study. Two radiologists independently reviewed both sets of images at separate sessions. Axial T2WI and multi-planar imaging of 3D T2WI were visually assessed for the presence of globe flattening. The optic nerve sheath diameter (ONSD) was measured at a location 4 mm posterior to each globe on oblique coronal imaging reformatted from 3D T2WI.
RESULTS
There were significantly more globes showing posterior flattening on 3D T2WI (105/138 [76.1%]) than on 2D T2WI (27/138 [19.6%], P = 0.001). Inter-observer agreement was excellent for both 2D T2WI and 3D T2WI (Cohen's kappa = 0.928 and 0.962, respectively). Intra-class correlation coefficient for the ONSD was almost perfect (Cohen's kappa = 0.839). The globes with posterior flattening had significantly larger ONSD than those without on both 2D and 3D T2WI (P < 0.001; 6.14 mm +/- 0.44 vs. 5.74 mm +/- 0.44 on 2D T2WI; 5.90 mm +/- 0.47 vs. 5.56 mm +/- 0.34 on 3D T2WI). Optic nerve protrusion was significantly more frequent on reformatted 1-mm 3D T2WI than on 5-mm 2D T2WI (8 out of 138 globes on 3D T2WI versus one on 2D T2WI; P = 0.018).
CONCLUSION
Posterior globe flattening is more frequently observed on 3D T2WI than on 2D T2WI in patients suspected of having increased intracranial pressure. The globes with posterior flattening have significantly larger ONSD than those without.
Keyword
Figure
-
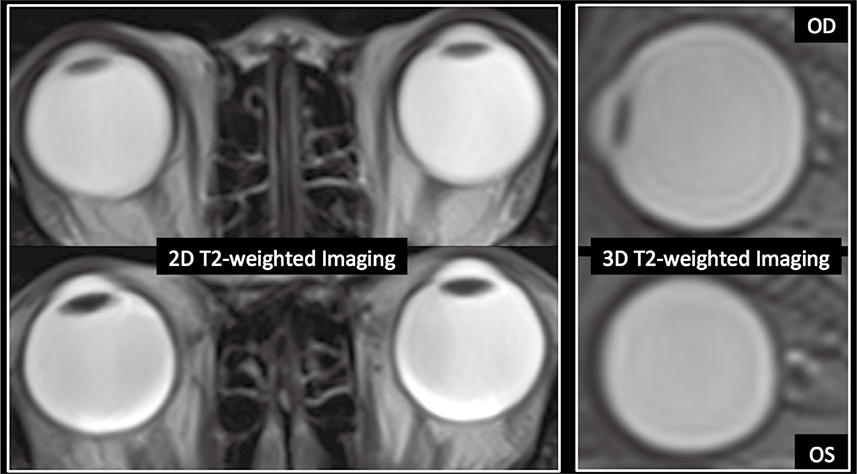
Fig. 1 2D transverse T2-weighted images and multiplanar-reformatted 3D T2-weighted images for visual assessment.

Fig. 2 Posterior globe flattening. Bilateral eye globes show straightening of the normal outward convexity of the sclera at the area of attachment to the optic nerve and mild indentation of posterior globes by a dilated optic nerve sheath (arrows).
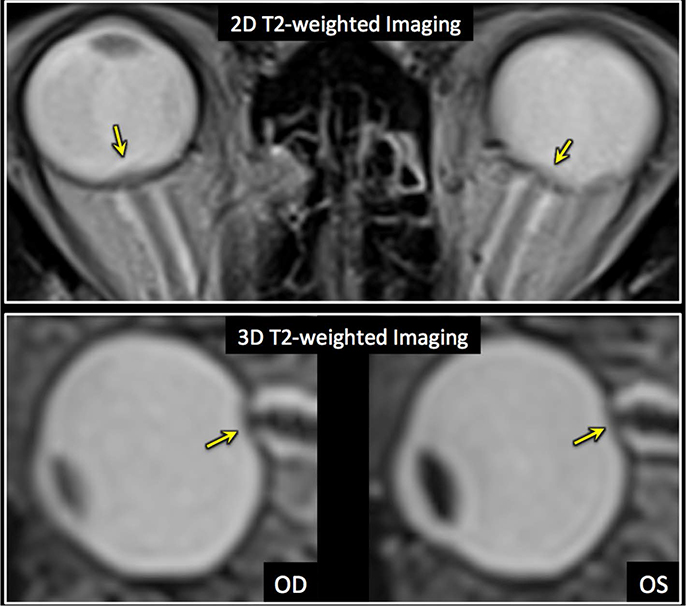
Fig. 3 Optic nerve protrusion is noted on both 2D and multiplanarreformatted 3D T2-weighted images (arrows), but more conspicuously visualized on 3D T2-weighted images.

Fig. 4 The optic nerve sheath diameter (hyperintense region, dashed arrows) is measured 4 mm posterior to the eye globe on multiplanar-reformatted 3D T2-weighted images.
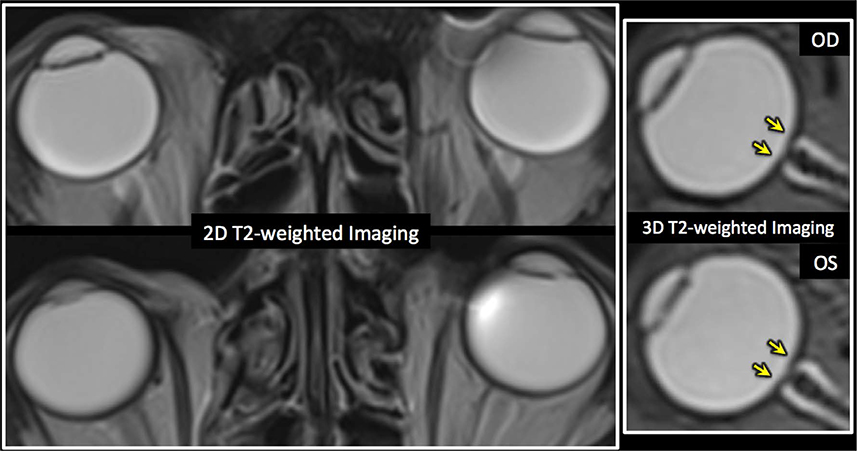
Fig. 5 Comparison of posterior globe flattening between 2D and 3D T2-weighted imaging. A 66-year-old male with acute infarcts in the bilateral frontal lobes and left parietal lobe shows posterior globe flattening on 3D T2-weighted imaging (arrows). However, it is not visible on 2D T2-weighted imaging.
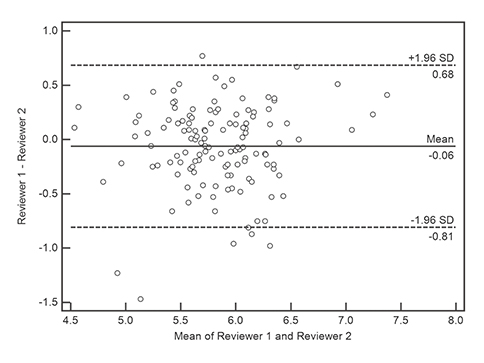
Fig. 6 Bland-Altman plot shows a slight bias between the two observers with mean differences ranging from -0.81 to 0.68.
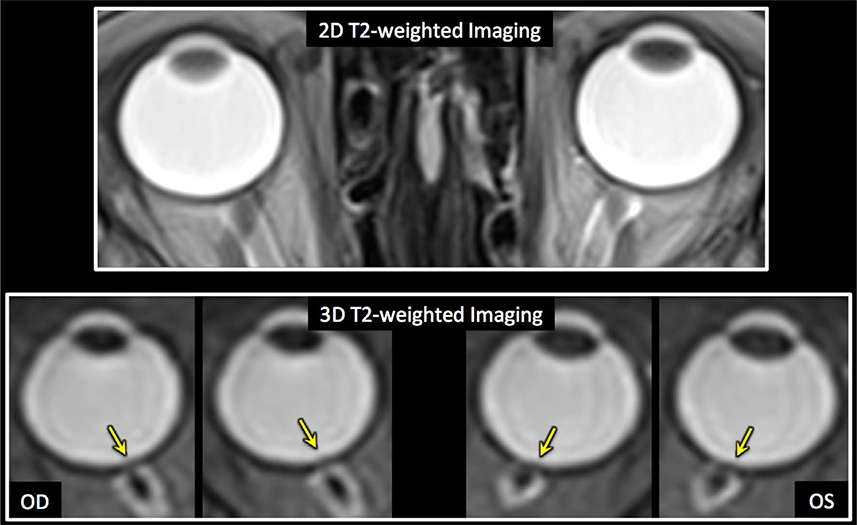
Fig. 7 Comparison of optic nerve protrusion between 2D and 3D T2-weighted imaging. A 70-year-old female with intracerebral hemorrhage shows optic nerve protrusion on both sides on 3D T2-weighted images (arrows). However, it is not noticeable on 2D T2-weighted images.
Reference
-
1. Ball AK, Clarke CE. Idiopathic intracranial hypertension. Lancet Neurol. 2006; 5:433–442.2. Binder DK, Horton JC, Lawton MT, McDermott MW. Idiopathic intracranial hypertension. Neurosurgery. 2004; 54:538–551. discussion 551-5323. Rohr AC, Riedel C, Fruehauf MC, et al. MR imaging findings in patients with secondary intracranial hypertension. AJNR Am J Neuroradiol. 2011; 32:1021–1029.4. Skau M, Brennum J, Gjerris F, Jensen R. What is new about idiopathic intracranial hypertension? An updated review of mechanism and treatment. Cephalalgia. 2006; 26:384–399.5. Algahtani HA, Baeesa SS, Obeid TH, Abuzinadah AR. Idiopathic intracranial hypertension. Atypical presentation. Saudi Med J. 2007; 28:762–765.6. Brodsky MC, Vaphiades M. Magnetic resonance imaging in pseudotumor cerebri. Ophthalmology. 1998; 105:1686–1693.7. Digre KB, Nakamoto BK, Warner JE, Langeberg WJ, Baggaley SK, Katz BJ. A comparison of idiopathic intracranial hypertension with and without papilledema. Headache. 2009; 49:185–193.8. Hansen HC, Helmke K. Validation of the optic nerve sheath response to changing cerebrospinal fluid pressure: ultrasound findings during intrathecal infusion tests. J Neurosurg. 1997; 87:34–40.9. Watanabe A, Kinouchi H, Horikoshi T, Uchida M, Ishigame K. Effect of intracranial pressure on the diameter of the optic nerve sheath. J Neurosurg. 2008; 109:255–258.10. Steffen H, Eifert B, Aschoff A, Kolling GH, Volcker HE. The diagnostic value of optic disc evaluation in acute elevated intracranial pressure. Ophthalmology. 1996; 103:1229–1232.11. Agid R, Farb RI, Willinsky RA, Mikulis DJ, Tomlinson G. Idiopathic intracranial hypertension: the validity of cross-sectional neuroimaging signs. Neuroradiology. 2006; 48:521–527.12. Sotoudeh H, Bowerson M, Parsons M, et al. Effect of spatial resolution of T2-weighted imaging on diagnostic efficacy of MRI in detection of papilledema. AJR Am J Roentgenol. 2015; 204:602–607.13. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977; 33:159–174.14. Hayreh SS. Pathogenesis of Oedema of the Optic Disc (Papilloedema). A Preliminary Report. Br J Ophthalmol. 1964; 48:522–543.15. Friedman DI. The pseudotumor cerebri syndrome. Neurol Clin. 2014; 32:363–396.16. Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002; 59:1492–1495.17. Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013; 81:1159–1165.18. Seitz J, Held P, Strotzer M, et al. Magnetic resonance imaging in patients diagnosed with papilledema: a comparison of 6 different high-resolution T1- and T2(*)-weighted 3-dimensional and 2-dimensional sequences. J Neuroimaging. 2002; 12:164–171.19. Alperin N, Bagci AM, Lam BL, Sklar E. Automated quantitation of the posterior scleral flattening and optic nerve protrusion by MRI in idiopathic intracranial hypertension. AJNR Am J Neuroradiol. 2013; 34:2354–2359.
