Effect of Manganese Content on the Magnetic Susceptibility of Ferrous-Manganese Alloys: Correlation between Microstructure on X-Ray Diffraction and Size of the Low-Intensity Area on MRI
- Affiliations
-
- 1Department of Radiology, Catholic University of Daegu, School of Medicine, Daegu, Korea. ysw10adest@cu.ac.kr
- 2Department of Materials Science and Metallurgical Engineering, Kyungpook National University, Daegu, Korea.
- 3Department of Pathology, Catholic University of Daegu, School of Medicine, Daegu, Korea.
- 4Department of Radiology, Kyungpook National University, School of Medicine, Daegu, Korea.
- 5Korea Institute of Industrial Technology Dongnam Technology Application Division, Pusan, Korea.
- KMID: 2175587
- DOI: http://doi.org/10.13104/imri.2015.19.2.76
Abstract
- PURPOSE
There is an ongoing search for a stent material that produces a reduced susceptibility artifact. This study evaluated the effect of manganese (Mn) content on the MRI susceptibility artifact of ferrous-manganese (Fe-Mn) alloys, and investigated the correlation between MRI findings and measurements of Fe-Mn microstructure on X-ray diffraction (XRD).
MATERIALS AND METHODS
Fe-Mn binary alloys were prepared with Mn contents varying from 10% to 35% by weight (i.e., 10%, 15%, 20%, 25%, 30%, and 35%; designated as Fe-10Mn, Fe-15Mn, Fe-20Mn, Fe-25Mn, Fe-30Mn, and Fe-35Mn, respectively), and their microstructure was evaluated using XRD. Three-dimensional spoiled gradient echo sequences of cylindrical specimens were obtained in parallel and perpendicular to the static magnetic field (B0). In addition, T1-weighted spin echo, T2-weighted fast spin echo, and T2*-weighted gradient echo images were obtained. The size of the low-intensity area on MRI was measured for each of the Fe-Mn binary alloys prepared.
RESULTS
Three phases of alpha'-martensite, gamma-austenite, and epsilon-martensite were seen on XRD, and their composition changed from alpha'-martensite to gamma-austenite and/or epsilon-martensite, with increasing Mn content. The Fe-10Mn and Fe-15Mn specimens comprised alpha'-martensite, the Fe-20Mn and Fe-25Mn specimens comprised gamma+epsilon phases, and the Fe-30Mn and Fe-35Mn specimens exhibited a single gamma phase. The size of the low-intensity areas of Fe-Mn on MRI decreased relative to its microstructure on XRD with increasing Mn content.
CONCLUSION
Based on these findings, proper conditioning of the Mn content in Fe-Mn alloys will improve its visibility on MR angiography, and a Mn content of more than 25% is recommended to reduce the magnetic susceptibility artifacts on MRI. A reduced artifact of Fe-Mn alloys on MRI is closely related to the paramagnetic constitution of gamma-austenite and/or epsilon-martensite.
Keyword
MeSH Terms
Figure
-
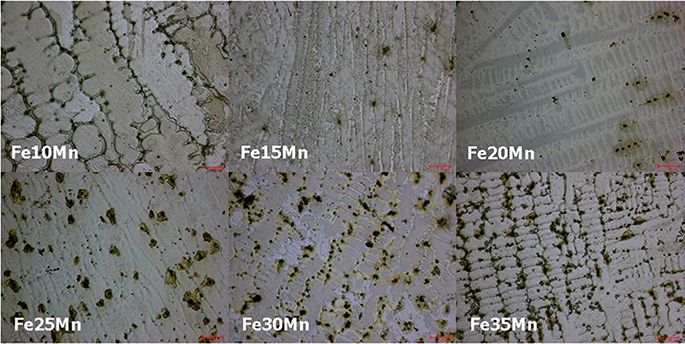
Fig. 1 Optical micrographs (× 100) of arc-melted ingots with the nominal compositions (i.e., 10%, 15%, 20%, 25%, 30%, and 35% Mn by weight; designated as Fe-10Mn, Fe-15Mn, Fe-20Mn, Fe-25Mn, Fe-30Mn, and Fe-35Mn, respectively). A typical dendritic structure was observed with zones of Mn aggregation between dendritic arms. Bar = 100 µm.
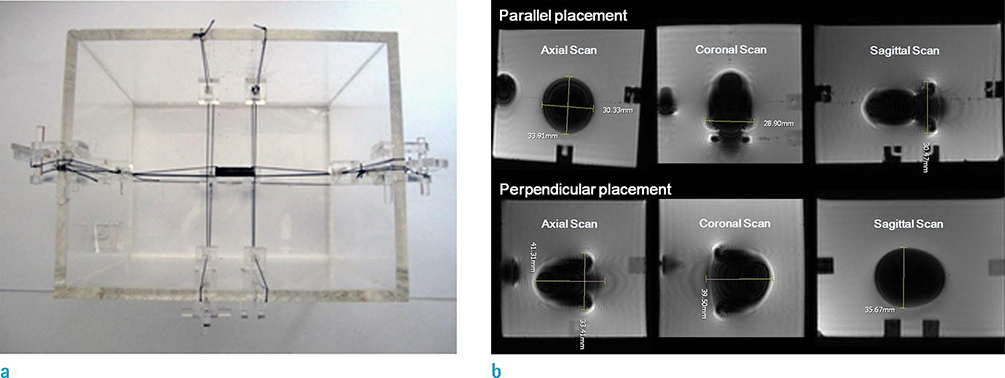
Fig. 2 Acquisition of MR images for various specimen locations and scanning planes, and measurement of the susceptibility artifact. (a) Photograph of the device designed for fixing the specimen to yield an MR image without disturbing the adjacent material in any plane. The cylindrical alloy rod was fixed in position with a polyester string within a container filled with CuSO4 solution. (b) The cylindrical rod (Fe25Mn; 4 mm × 15 mm) was placed parallel (upper row) or perpendicular (lower row) to B0. Three-dimensional spoiled gradient echo sequences (3D SPGR) were obtained in the axial, coronal, and sagittal planes, in that order. The maximum diameter of the resulting hypointensity was measured on a picture archiving system to assess the size of the susceptibility artifact.
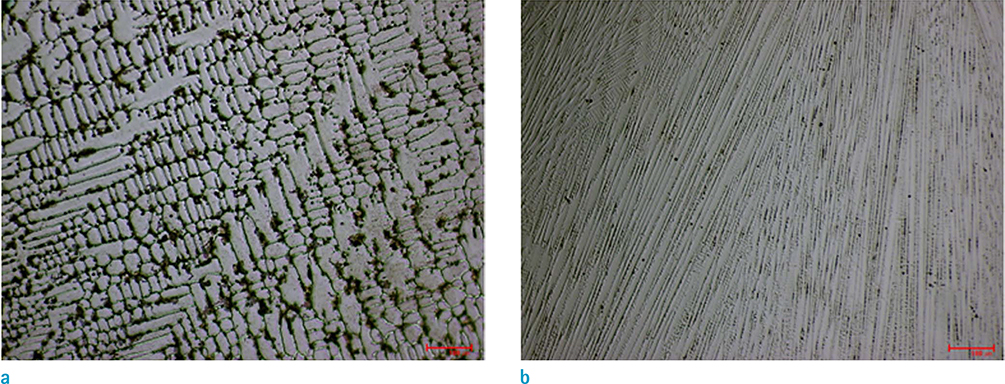
Fig. 3 Optical micrographs (× 100) of specimens with the nominal compositions Fe65Mn35 specimens (wt %). (a) Arc-melted ingots, (b) suction-cast specimens. Very fine dendrite structures were formed, with dendrites having a relatively high Mn content being formed due to a relatively high solidification rate during suction casting. Bar = 100 µm.

Fig. 4 Microhardness of the (a) arc-melted and (b) suction-cast specimens with the nominal compositions Fe100-xMnx (wt %). The hardness values were > 200 HV for the samples with an Mn content of < 30%.
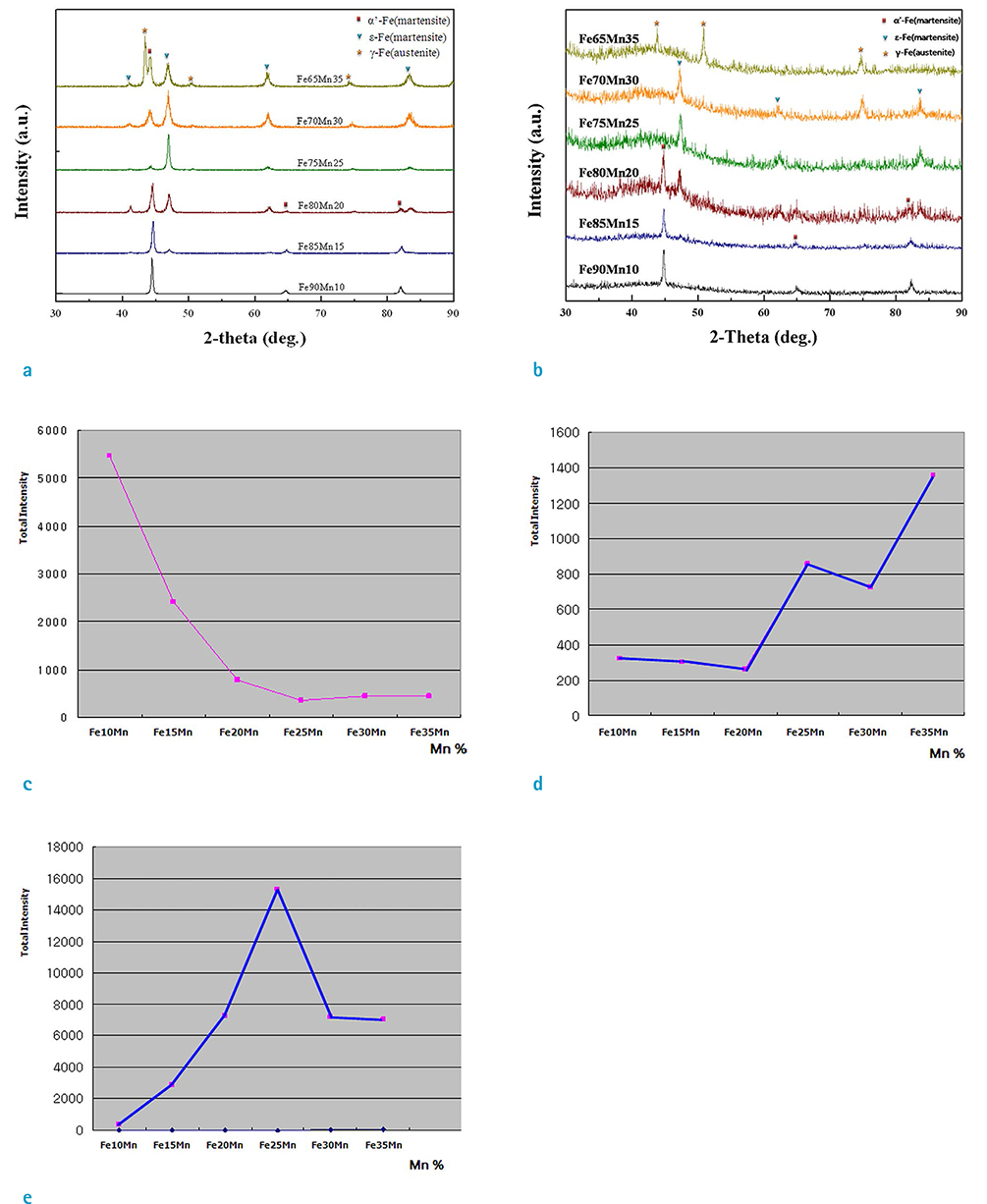
Fig. 5 The XRD spectra of (a) arc-melted ingots and (b) suction-cast specimens with the nominal compositions Fe100-xMnx (wt %) showing the phase identification and distribution. Diffraction peaks corresponding to α'-martensite (rectangle), γ-austenite (asterisk), and ε-martensite (triangle) are indicated. The amplitudes of the peaks found at positions corresponding to the 2-θ interval of (c) α'-martensite (63.0-66.0°), (d) γ-austenite (49.0-52.0°), and (e) ε-martensite (46.0-48.0°) can be observed to differ with the alloy Mn content.
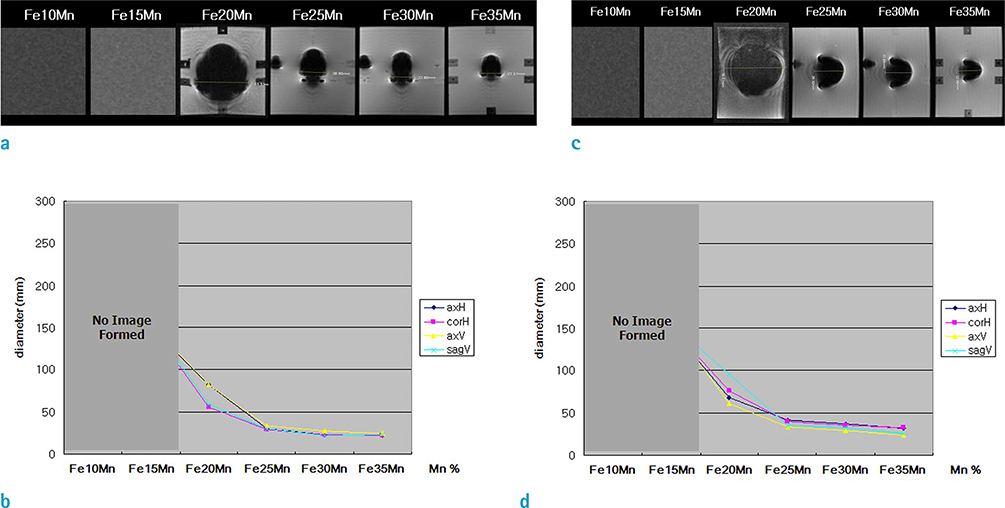
Fig. 6 The low-intensity area of the Fe-Mn alloys on 3D SPGR according to Mn content. The cylindrical specimen (4 × 15 mm) was placed either parallel (a, b) or perpendicular (c, d) to B0. The size of the low-intensity area decreased rapidly between, as the Mn content increased from 20% to 25%, and reached a plateau at 30-35% in both conditions. The horizontal (axH) and vertical (axV) maximum diameters were measured in the axial scanning planes. The horizontal (corH) and vertical (sagV) maximum diameters were measured in the coronal and sagittal planes.

Fig. 7 Susceptibility artifacts on various MRI sequences for different alloy Mn contents, and with or without homogenization heat treatment (HT). (a) T1WI (first row), T2WI (second row), 3D SPGR (third row), and T2*-GRE (fourth row) of a 2.5 mm × 20 mm cylindrical rod parallel to B0. (b) Length ratio (length of maximum low-intensity area in mm/actual length of 20 mm) and (c) diameter ratio (diameter of maximum low-intensity area in mm/actual diameter of 2.5 mm) showing that the susceptibility artifact decreased rapidly for 20-25% Mn, and reached a plateau for 30% Mn. The HT decreased the size of the low-intensity area for 20% Mn but not for 25-30% Mn. 20NH (Mn 20% without HT); 20HT (Mn 20% with HT); 25NH (Mn 25% without HT); 25HT (Mn 25% with HT); 30NH (Mn 30% without HT); 30HT (Mn 30% with HT).
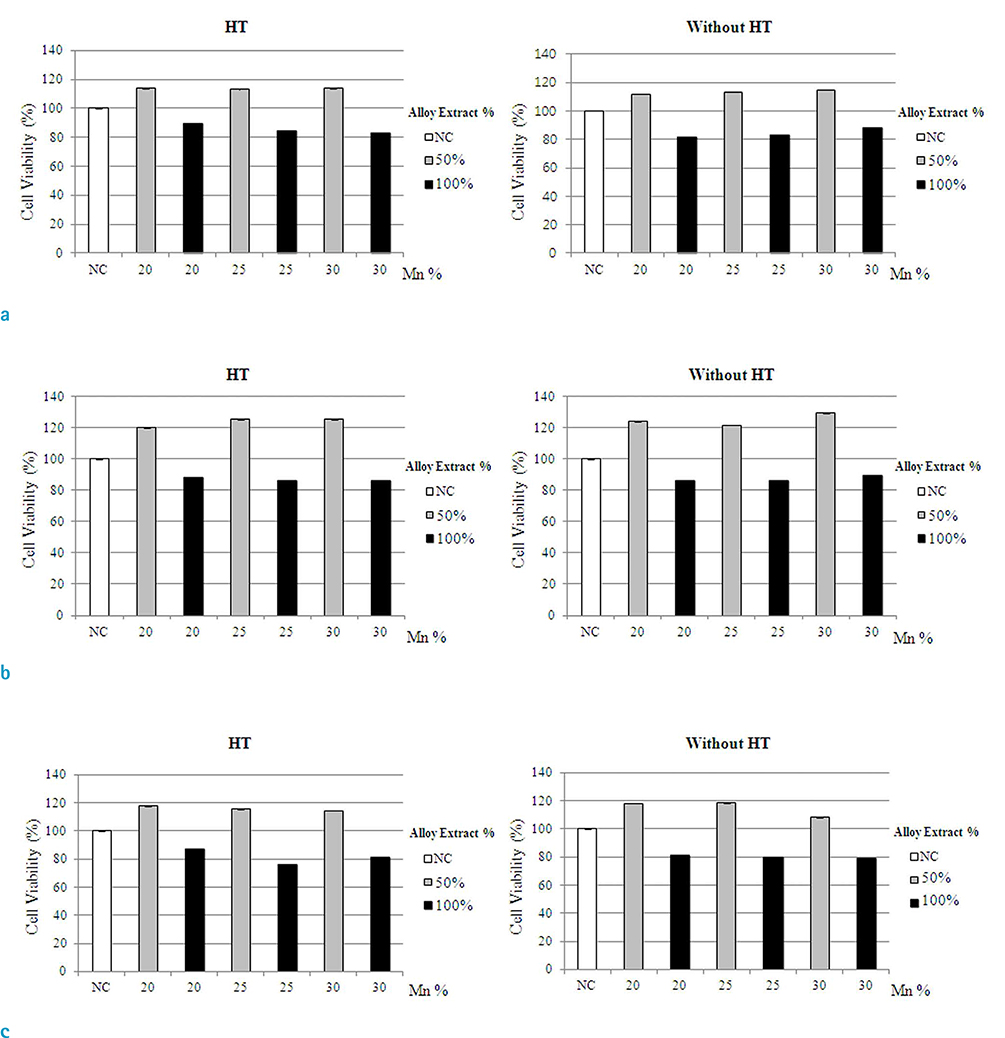
Fig. 8 MTT assays according to Mn content and HT at alloy extract concentrations of 50% and 100%. The cell viability for each Mn content (i.e., 20%, 25%, and 30%) was estimated to be 80-90% at day 1 (a) and day 2 (b), and 70-80% on day 4 (c). NC = normal control
Reference
-
1. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med. 1987; 316:701–706.2. Schomig A, Kastrati A, Mudra H, et al. Four-year experience with Palmaz-Schatz stenting in coronary angioplasty complicated by dissection with threatened or present vessel closure. Circulation. 1994; 90:2716–2724.3. Hoffmann R, Mintz GS, Dussaillant GR, et al. Patterns and mechanisms of in-stent restenosis. A serial intravascular ultrasound study. Circulation. 1996; 94:1247–1254.4. Heublein B, Rohde R, Kaese V, Niemeyer M, Hartung W, Haverich A. Biocorrosion of magnesium alloys: a new principle in cardiovascular implant technology? Heart. 2003; 89:651–656.5. Waksman R, Pakala R, Kuchulakanti PK, et al. Safety and efficacy of bioabsorbable magnesium alloy stents in porcine coronary arteries. Catheter Cardiovasc Interv. 2006; 68:607–617. discussion 618-6196. Waksman R. Update on bioabsorbable stents: from bench to clinical. J Interv Cardiol. 2006; 19:414–421.7. Erne P, Schier M, Resink TJ. The road to bioabsorbable stents: reaching clinical reality? Cardiovasc Intervent Radiol. 2006; 29:11–16.8. Peuster M, Wohlsein P, Brugmann M, et al. A novel approach to temporary stenting: degradable cardiovascular stents produced from corrodible metal-results 6-18 months after implantation into New Zealand white rabbits. Heart. 2001; 86:563–569.9. Peuster M, Hesse C, Schloo T, Fink C, Beerbaum P, von Schnakenburg C. Long-term biocompatibility of a corrodible peripheral iron stent in the porcine descending aorta. Biomaterials. 2006; 27:4955–4962.10. Hermawan H, Dube D, Mantovani D. Degradable metallic biomaterials: design and development of Fe-Mn alloys for stents. J Biomed Mater Res A. 2010; 93:1–11.11. Schinhammer M, Hanzi AC, Loffler JF, Uggowitzer PJ. Design strategy for biodegradable Fe-based alloys for medical applications. Acta Biomater. 2010; 6:1705–1713.12. Liu B, Zheng YF. Effects of alloying elements (Mn, Co, Al, W, Sn, B, C and S) on biodegradability and in vitro biocompatibility of pure iron. Acta Biomater. 2011; 7:1407–1420.13. Buecker A, Spuentrup E, Ruebben A, Gunther RW. Artifact-free in-stent lumen visualization by standard magnetic resonance angiography using a new metallic magnetic resonance imaging stent. Circulation. 2002; 105:1772–1775.14. Trost DW, Zhang HL, Prince MR, et al. Three-dimensional MR angiography in imaging platinum alloy stents. J Magn Reson Imaging. 2004; 20:975–980.15. O'Brien BJ, Stinson JS, Boismier DA, Carroll WM. Characterization of an NbTaWZr alloy designed for magnetic resonance angiography compatible stents. Biomaterials. 2008; 29:4540–4545.16. O'Brien B, Stinson J, Carroll W. Development of a new niobium-based alloy for vascular stent applications. J Mech Behav Biomed Mater. 2008; 1:303–312.17. American Society for Testing and Materials (ASTM) standard F2119-07. Standard test method for evaluation of MR image artifacts from passive implants. 2013. Accessed June 19, 2015. http://www.astm.org/Standards/F2119.htm.18. Port JD, Pomper MG. Quantification and minimization of magnetic susceptibility artifacts on GRE images. J Comput Assist Tomogr. 2000; 24:958–964.19. Wang Y, Truong TN, Yen C, et al. Quantitative evaluation of susceptibility and shielding effects of nitinol, platinum, cobalt-alloy, and stainless steel stents. Magn Reson Med. 2003; 49:972–976.20. Coecke S, Balls M, Bowe G, et al. Guidance on good cell culture practice. a report of the second ECVAM task force on good cell culture practice. Altern Lab Anim. 2005; 33:261–287.21. Gu X, Zheng Y, Cheng Y, Zhong S, Xi T. In vitro corrosion and biocompatibility of binary magnesium alloys. Biomaterials. 2009; 30:484–498.22. Choi JW, Roh HG, Moon WJ, et al. Time-resolved 3D contrast-enhanced MRA on 3.0T: a non-invasive follow-up technique after stent-assisted coil embolization of the intracranial aneurysm. Korean J Radiol. 2011; 12:662–670.23. Takayama K, Taoka T, Nakagawa H, et al. Usefulness of contrast-enhanced magnetic resonance angiography for follow-up of coil embolization with the enterprise stent for cerebral aneurysms. J Comput Assist Tomogr. 2011; 35:568–572.24. Seok JH, Choi HS, Jung SL, et al. Artificial luminal narrowing on contrast-enhanced magnetic resonance angiograms on an occasion of stent-assisted coiling of intracranial aneurysm: in vitro comparison using two different stents with variable imaging parameters. Korean J Radiol. 2012; 13:550–556.25. Crossgrove J, Zheng W. Manganese toxicity upon overexposure. NMR Biomed. 2004; 17:544–553.26. Reaney SH, Bench G, Smith DR. Brain accumulation and toxicity of Mn(II) and Mn(III) exposures. Toxicol Sci. 2006; 93:114–124.27. Chang Y, Jin SU, Kim Y, et al. Decreased brain volumes in manganese-exposed welders. Neurotoxicology. 2013; 37:182–189.28. Chen JY, Tsao GC, Zhao Q, Zheng W. Differential cytotoxicity of Mn(II) and Mn(III): special reference to mitochondrial [Fe-S] containing enzymes. Toxicol Appl Pharmacol. 2001; 175:160–168.29. Hermawan H, Purnama A, Dube D, Couet J, Mantovani D. Fe-Mn alloys for metallic biodegradable stents: degradation and cell viability studies. Acta Biomater. 2010; 6:1852–1860.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study on the Manganese Exposure and Health Hazard among Manganese Manufacturing Woman Workers
- Significance of Brain Magnetic Resonance Imaging (MRI) in the Assessment of Occupational Manganese Exposure
- Study on Clinical Significance of High Signal Intensity by Brain Magnetic Resonance Imaging in Mild Steel/Arc Welders (Clinical Significance of High Signal Intensity by Brain MRI in Welders)
- Relationship of Biological Indices of Manganese with Pallidal Index on MRI in Liver Cirrhotics
- The Change of Brain MRI and Pathology According to the Administered Dose of Manganese in Rats
