Immediate Conservative Breast Reconstruction Technique using Lateral Thoracodorsal Fasciocutaneous Flap
- Affiliations
-
- 1Department of Surgery, College of Medicine, Pusan National University, Busan, Korea. bytae@hyowon.pusan.ac.kr
- KMID: 2175039
- DOI: http://doi.org/10.4048/jbc.2007.10.3.217
Abstract
-
PURPOSE: A lateral thoracodorsal fasciocutaneous flap (LTFF) is a local fasciocutaneous flap that has been used in breast reconstructions since the 1980s. Although the LTFF is a wellstudied reconstruction procedure after radical surgery in Western countries, there is no report in Korea. By introducing the LTFF procedure, we suggest an easy reconstruction technique that can be performed by the breast surgeon directly.
METHODS
Patients with lateral breast cancer and redundant lateral thoracic region might be candidates for this procedure. The flap consists of the lateral and dorsal extensions of the inframammarian fold as well as an extended line from the anterior axillary line. A quadrantectomy is performed through a planned skin incision, and an axillary lymph node dissection can be performed simultaneously if the sentinel lymph node is positive. The skin and subcutaneous fat with the fascia of the serratus anterior and latissimus dorsi muscle should be dissected carefully. A wedge-shaped flap can be acquired successfully. The lateral breast defect is then reconstructed by a rotation of the flap. The axis of the flap is drawn following the inframammarian fold so that the final scar would be under the brassiere line.
RESULTS
Nineteen patients were treated with the LTFF after breast conserving surgery. All tumors were located in lateral breast regions. Seroma occurred in three and partial fat necrosis and partial flap necrosis were observed in each one. The cosmetic result based on four-point scoring system of breast cosmesis showed excellent in seventeen and good in two.
CONCLUSION
Despite its long scar line, with appropriate patient selection, a LTFF might be a useful method for breast reconstructions.
MeSH Terms
Figure
-

Fig 1 Flap design. The design of flap is consisted of the lateral and dorsal extensions of the inframammarian fold and a line extended from the anterior axillary line. The extension of the inframammarian fold can reach the posterior thoracic region, and extension of the anterior axillary line is designed more obliquely with curved border.
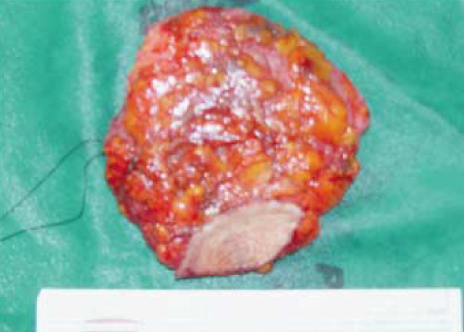
Fig 2 Resected breast cancer. Quadrantectomy and axillary lymph node dissection, if sentinel lymph node biopsy is positive, is performed through a planned skin incision.

Fig 3 The prepared lateral thoracodorsal fasciocutaneous flap. The skin and subcutaneous fat with fascia of serratus anterior and latissimus dorsi muscle are carefully dissected. We can acquire the wedge-shaped LTFF. Vascular feeding of the flap is from the fascia of underlying muscles. The careful dissection from the underlying muscles may protect the partial flap loss and fat necrosis.

Fig 4 Completed reconstruction. A lateral breast defect is reconstructed by a rotation of LTFF. The LTFF axis is drawn following the inframammarian fold, so that the final scar will be under the brassiere line.
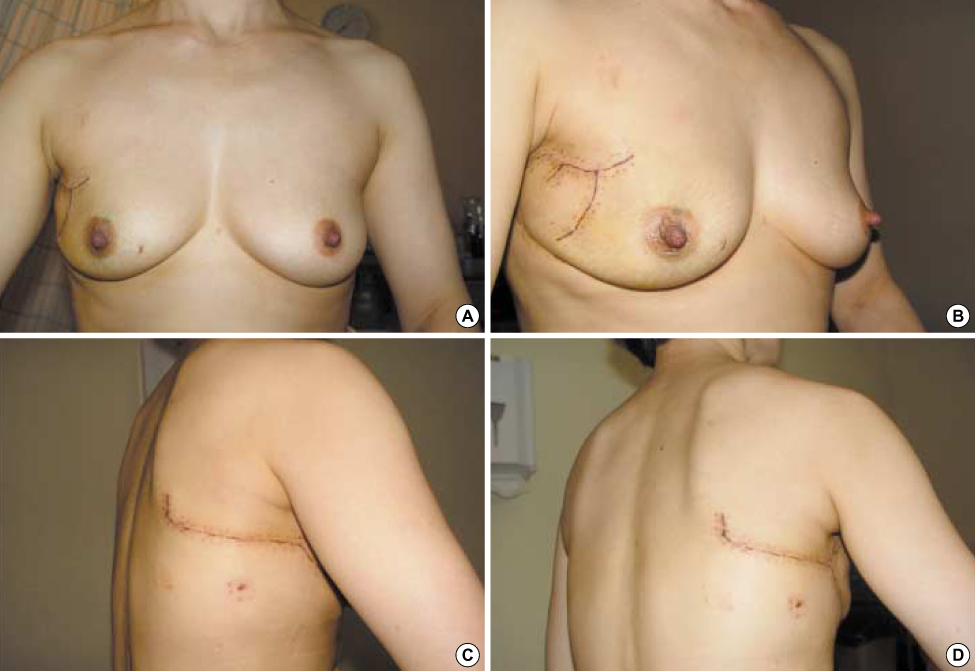
Fig 5 Postoperative reconstruction state. After discharge, postoperative wound healing is observed. In this patient, she visited outpatient clinics at postoperative day 11 with all staples and drain removed. (A) Anterior view, (B) Anterior oblique view, (C) Lateral view, (D) Posterior oblique view.
Cited by 2 articles
-
Immediate Breast Reconstruction with Contralateral Pectoralis Major Myomammary Flap for Breast Conserving Surgery
Seung Ju Lee, Young Tae Bae, Hyong Il Seo, Tae Woo Kang
J Breast Cancer. 2008;11(4):206-212. doi: 10.4048/jbc.2008.11.4.206.Oncoplastic Breast Surgery
Young-tae Bae
J Korean Med Assoc. 2009;52(10):981-995. doi: 10.5124/jkma.2009.52.10.981.
Reference
-
1. Slavin SA, Halperin T. Reconstruction of the breast conservation deformity. Seminars Plast Surg. 2004. 18:89–96.
Article2. Clough KB, Kroll SE, Audretsch W. An approach to the repair of partial mastectomy defects. Plast Reconstr Surg. 1999. 104:409–420.
Article3. Kroll SS, Singletary SE. Repair of partial of mastectomy defects. Clin Plast Surg. 1998. 25:303–310.4. Germann G, Steinau HU. Breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 1996. 97:519–526.
Article5. Chang DW, Youssef A, Cha S, Reece GP. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 2002. 110:751–759.
Article6. Hartrampf CR, Scheflan M, Black PW. Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg. 1982. 69:216–225.
Article7. Watterson PA, Bostwick Jr III, Hester TR Jr. TRAM flap anatomy correlated with a 10-year clinical experience with 556 pateints. Plast Reconstr Surg. 1995. 95:1185–1194.
Article8. Allen RJ, Treece P. Deep inferior epigastric perforator flap for breast reconstruction. Ann Plast Surg. 1994. 32:32–38.
Article9. DellaCroce FJ, Sullivan SK. Application and refinement of the superior gluteal artery perforator free flap for bilateral simultaneous breast reconstruction. Plast Reconstr Surg. 2005. 116:97–103.
Article10. Allen RJ, Levine JL, Granzow JW. The in-the-crease inferior gluteal artery perforator flap for breast reconstruction. Plast Reconstr Surg. 2006. 118:333–339.
Article11. Clough KB, Nos C, Salmon RJ, Soussaline M, Durand JC. Conservative treatment of breast cancer by mammaplasty and irradiation: A new approach to lower quadrant tumors. Plast Reconstr Surg. 1995. 96:363–370.12. Newman LA, Kuerer HM, McNeese MD, Hunt KK, Gurtner GC, Vlastos GS, et al. Reduction mammoplasty improves breast conservation therapy in patients with macromastia. Am J Surg. 2001. 181:215–220.
Article13. Spear SL, Pelletiere CV, Wolfe AJ, Tsangaris TN, Pennanen MF. Experience with reduction mammaplasty combined with breast conservation therapy in the treatment of breast cancer. Plast Reconstr Surg. 2003. 111:1102–1109.
Article14. Chang E, Johnson N, Webber B, Booth J, Rahhal D, Gannett D, et al. Bilateral reduction mammoplasty in combination with lumpectomy for treatment of breast cancer in patients with macromastia. Am J Surg. 2004. 187:647–650.
Article15. Holmstrom H, Lossing C. The lateral thoracodorsal flap in breast reconstruction. Plast Reconstr Surg. 1986. 77:933–943.
Article16. Blomqvist L, Malm M. Clinical experience with the lateral thoracodorsal flap in breast reconstruction. Ann Plast Surg. 1999. 43:7–13.
Article17. Blomqvist L, Malm M, Holmstrom H, Lossing C. The lateral thoracodorsal flap in breast reconstruction: a comparison between two plastic surgical centres. Scand J Plast Reconstr Hand Surg. 2000. 34:331–338.18. Monica M, Eric AS, Lawrence WB, David D, Barbara F, Armando G, et al. Standard for breast bonservation therapy in the management of invasive breast carcinoma. CA Cancer J Clin. 2002. 52:277–300.19. Bae YC, Kim SH, Kim JH, Bae YT. A study on the perception of breast reconstruction in mastectomized patients and general population in Korea. J Korean Soc Plast Reconstr Surg. 1997. 24:1062–1075.20. Lossing C, Elander A, Gewalli F. The lateral thoracodorsal flap in breast reconstruction: a long term follow up study. Scand J Plast Reconstr Hand Surg. 2001. 35:183–192.
Article21. Hudson DA. Aesthetic modification for delayed autologous breast reconstruction: using a thoracodorsal flap to create a breast pocket. Ann Plast Surg. 2001. 47:589–593.
Article22. Woerdeman L, van Schijndel A, Hage JJ, Smeulders M. Verifying surgical results and risk factors of the lateral thoracodorsal flap. Plast Reconstr Surg. 2004. 113:196–203.
Article23. de Weerd L, Woerderman LA, Hage JJ. The lateral thoracodorsal flap as a salvage procedure for partial transverse rectus abdominis myocutaneous or deep inferior epigastric perforator flap loss in breast reconstruction. Ann Plast Surg. 2005. 54:590–594.
Article24. Munhoz AM, Montag E, Arruda EG, Aldrighi C, Gemperli R, Aldrighi JM, et al. The role of the lateral thoracodorsal fasciocutaneous flap in immediate conservative breast surgery reconstruction. Plast Reconstr Surg. 2006. 117:1699–1710.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of a Lateral Thoracodorsal Flap after Breast Conserving Surgery in Laterally Located Breast Cancer
- The Lateral Thoracodorsal Flap in Delayed Bilateral Breast Reconstruction for an Obese Patient with Redundant Lateral Chest Wall Soft Tissue
- Thoracodorsal artery flaps for breast reconstruction–the variants and its approach
- Nipple Reconstruction using the C-V Flap Technique after Breast Reconstruction with the Only Breast Expander
- Vulvoperineal Reconstruction Using Various Fasciocutaneous Flaps
