Chonnam Med J.
2014 Dec;50(3):112-114. 10.4068/cmj.2014.50.3.112.
Thrombotic Occlusion during Intravascular Ultrasonography-Guided Percutaneous Coronary Intervention of Stumpless Chronic Total Occlusion
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyung Hee University Hospital, Kyung Hee University, Seoul, Korea. mylovekw@hanmail.net
- KMID: 2172155
- DOI: http://doi.org/10.4068/cmj.2014.50.3.112
Abstract
- Percutaneous coronary intervention (PCI) of stumpless chronic total occlusion (CTO) lesions with a side branch stemming from the occlusion have a significantly lower treatment success rate because physicians cannot identify an accurate entry point with only conventional angiographic images. An intravascular ultrasonography (IVUS)-guided wiring technique might be useful for the penetration of stumpless CTO. We recently experienced thrombotic occlusion during an IVUS-guided stumpless CTO procedure. The cause of the thrombosis is not completely understood; the thrombosis may have been associated with the long use of the IVUS catheter. Special precautions should be taken to prevent thrombus in such cases.
Figure
-

FIG. 1 Coronary angiographic findings during the PCI. (A) The intact left anterior descending artery (LAD) is shown 2 years previously by the white arrowhead in spider view. (B) At admission, the LAD is in a stumpless chronic total occlusion state with a side branch arising from the LAD ostium. (C) Diffuse thrombosis at the ramus intermedius 30 minutes after the IVUS-guided procedure. The thrombotic lesion is indicated by black arrows. (D) The final angiogram after thrombus aspiration and intracoronary abciximab bolus injection.
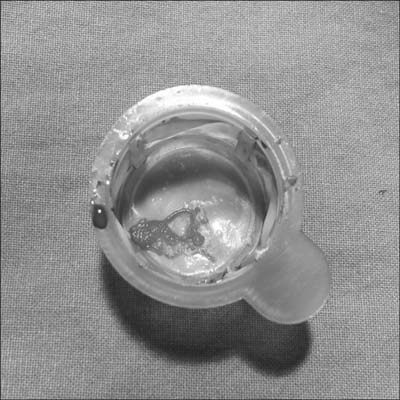
FIG. 2 Large red thrombus from the aspiration catheter.
Reference
-
1. Fefer P, Knudtson ML, Cheema AN, Galbraith PD, Osherov AB, Yalonetsky S, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012; 59:991–997.2. Melchior JP, Doriot PA, Chatelain P, Meier B, Urban P, Finci L, et al. Improvement of left ventricular contraction and relaxation synchronism after recanalization of chronic total coronary occlusion by angioplasty. J Am Coll Cardiol. 1987; 9:763–768.
Article3. Warren RJ, Black AJ, Valentine PA, Manolas EG, Hunt D. Coronary angioplasty for chronic total occlusion reduces the need for subsequent coronary bypass surgery. Am Heart J. 1990; 120:270–274.
Article4. Fujii K, Ochiai M, Mintz GS, Kan Y, Awano K, Masutani M, et al. Procedural implications of intravascular ultrasound morphologic features of chronic total coronary occlusions. Am J Cardiol. 2006; 97:1455–1462.
Article5. Park Y, Park HS, Jang GL, Lee DY, Lee H, Lee JH, et al. Intravascular ultrasound guided recanalization of stumpless chronic total occlusion. Int J Cardiol. 2011; 148:174–178.
Article6. Grayburn PA, Willard JE, Brickner ME, Eichhorn EJ. In vivo thrombus formation on a guidewire during intravascular ultrasound imaging: evidence for inadequate heparinization. Cathet Cardiovasc Diagn. 1991; 23:141–143.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iteration of Reverse Controlled Antegrade and Retrograde Tracking for Coronary Chronic Total Occlusion Intervention: a Current Appraisal
- Two Cases of Complications during Percutaneous Coronary Intervention for Myocardial Infarction in Patients with Concurrent Chronic Total Occlusion in an Emergency Setting
- Reverse Controlled Antegrade and Retrograde Subintimal Tracking in Chronic Total Occlusion of Right Coronary Artery
- Intravascular Ultrasound-Guided Troubleshooting in a Large Hematoma Treated With Fenestration Using a Cutting Balloon
- Interventional Management of “Balloon-Uncrossable†Coronary Chronic Total Occlusion: Is There Any Way Out?
