Totally Occluded Grafted Right Internal Mammary Artery to Anomalously Originated Right Coronary Artery
- Affiliations
-
- 1Division of Cardiology of Chonnam National University Hospital, Cardiovascular Convergence Research Center Nominated by Korea Ministry of Health and Welfare, Gwangju, Korea. hyj200@hanmail.net
- KMID: 2172147
- DOI: http://doi.org/10.4068/cmj.2015.51.1.43
Abstract
- An anomalous aortic origin of a coronary artery is rare and surgical intervention is recommended when the patient is symptomatic. We performed coronary artery bypass graft surgery in a 21-year-old male patient with a right coronary artery anomalously originating from the left coronary sinus. The artery was significantly stenosed by external compression between the aorta and the pulmonary artery. However, the graft became occluded 1 year after the operation. In such cases, the dynamic nature of the stenosis can cause relatively intact antegrade competitive flow from the native coronary artery and lead to an occlusion of the grafted artery. Methods for evaluating flow rates or intraluminal pressures of native arteries could be helpful in decision-making in similar cases.
MeSH Terms
Figure
-

FIG. 1 Cardiac Computed Tomography Angiography. The right coronary artery is originated from the left coronary sinus (blue long arrow) and was trapped between the aorta (red short arrow) and the pulmonary artery (yellow arrowhead).
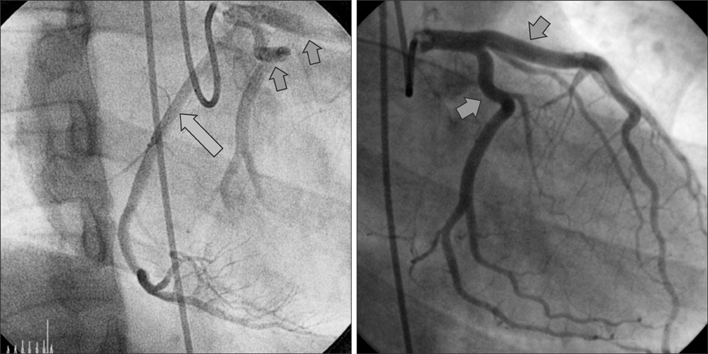
FIG. 2 Coronary angiography showed that both the right coronary artery (blue long arrow) and the left coronary arteries (red short arrows) originated from the left coronary sinus simultaneously, suggesting an anomalously originating RCA (left image). The left coronary arteries are normal (right image).
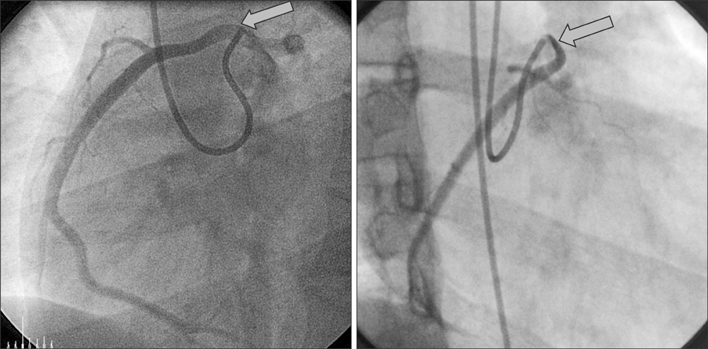
FIG. 3 The right coronary artery seems to be normal in the left anterior oblique view (left image), but in the right anterior oblique view, significant stenosis in the proximal RCA due to external compression is shown (right image, blue arrow).
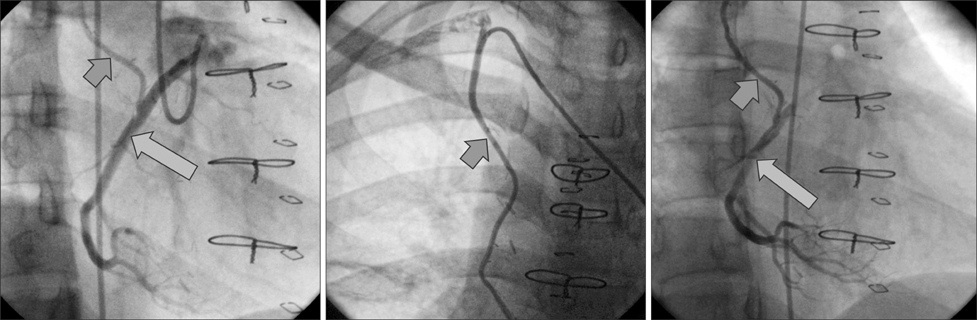
FIG. 4 After coronary artery bypass grafting surgery, a patent right internal mammary artery (red short arrow) to the right coronary artery (blue long arrow) is noted.
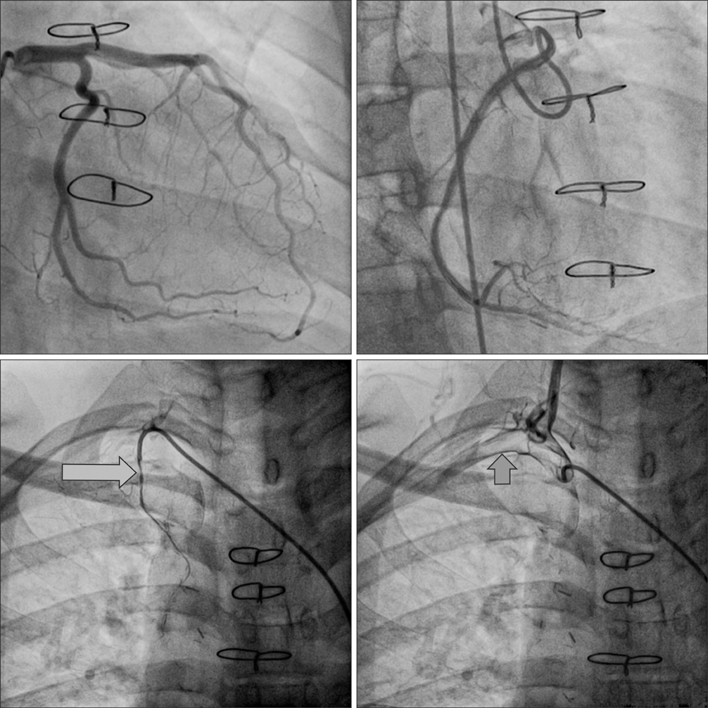
FIG. 5 One year after coronary artery bypass graft surgery, the right internal mammary artery was totally occluded (blue long arrow), whereas the 3 coronary arteries were unchanged (upper 2 images) and the right subclavian artery was intact (short red arrow).
Reference
-
1. Davis JA, Cecchin F, Jones TK, Portman MA. Major coronary artery anomalies in a pediatric population: incidence and clinical importance. J Am Coll Cardiol. 2001; 37:593–597.
Article2. Maron BJ, Carney KP, Lever HM, Lewis JF, Barac I, Casey SA, et al. Relationship of race to sudden cardiac death in competitive athletes with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2003; 41:974–980.
Article3. Eckart RE, Scoville SL, Campbell CL, Shry EA, Stajduhar KC, Potter RN, et al. Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med. 2004; 141:829–834.
Article4. Gersony WM. Management of anomalous coronary artery from the contralateral coronary sinus. J Am Coll Cardiol. 2007; 50:2083–2084.
Article5. Brothers JA, McBride MG, Seliem MA, Marino BS, Tomlinson RS, Pampaloni MH, et al. Evaluation of myocardial ischemia after surgical repair of anomalous aortic origin of a coronary artery in a series of pediatric patients. J Am Coll Cardiol. 2007; 50:2078–2082.
Article6. Tatoulis J, Buxton BF, Fuller JA. Patencies of 2127 arterial to coronary conduits over 15 years. Ann Thorac Surg. 2004; 77:93–101.
Article7. Berger A, MacCarthy PA, Siebert U, Carlier S, Wijns W, Heyndrickx G, et al. Long-term patency of internal mammary artery bypass grafts: relationship with preoperative severity of the native coronary artery stenosis. Circulation. 2004; 110:11 Suppl 1. II36–II40.8. Krasuski RA, Magyar D, Hart S, Kalahasti V, Lorber R, Hobbs R, et al. Long-term outcome and impact of surgery on adults with coronary arteries originating from the opposite coronary cusp. Circulation. 2011; 123:154–162.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preparation of the internal mammary artery graft in coronary artery surgery-comparison of free mammary artery flows
- Percutaneous Transluminal Angioplasty of a Stenosis of an Internal Mammary Artery Graft
- A Hybrid Procedure for Coronary Artery Disease with Left Subclavian Artery Stenosis
- The Angiographic Evaluation of Patency after Coronary Artery Bypass Graft
- The Effect of Thoracic Epidural Lidocaine on Blood Flow of Grafted Coronary Vessels in Coranary Artery Bypass Graft Surgery
