Comparative Analysis of the Mini-pterional and Supraorbital Keyhole Craniotomies for Unruptured Aneurysms with Numeric Measurements of Their Geometric Configurations
- Affiliations
-
- 1Department of Neurosurgery, Daegu Fatima Hospital, Daegu, Korea. paulyoonsoolee@hanmail.net
- KMID: 2172024
- DOI: http://doi.org/10.7461/jcen.2013.15.1.5
Abstract
OBJECTIVE
Keyhole craniotomy is a modification of pterional craniotomy that allows for use of a minimally invasive approach toward cerebral aneurysms. Currently, mini-pterional (MPKC) and supraorbital keyhole craniotomies (SOKC) are commonly used. In this study, we measured and compared the geometric configurations of surgical exposure provided by MPKC and SOKC.
METHODS
Nine patients underwent MPKC and four underwent SOKC. Their postoperative contrast-enhanced brain computed tomographic scans were evaluated. The transverse and longitudinal diameters and areas of exposure were measured. The locations of the anterior communicating artery, bifurcation of the middle cerebral artery (MCAB), and the internal carotid artery (ICA) terminal were identified, and the working angles and depths for these targets were measured.
RESULTS
No significant differences in the transverse diameters of exposure were observed between MPKC and SOKC. However, the longitudinal diameters and the areas were significantly larger, by 1.5 times in MPKC. MPKC provided larger operable working angles for the targets. The angles by MPKC, particularly for the MCAB, reached up to 1.9-fold of those by SOKC. Greater working depths were required in order to reach the targets by SOKC, and the differences were the greatest in the MCAB by 1.6-fold.
CONCLUSION
MPKC provides larger exposure than SOKC with a similar length of skin incision. MPKC allows for use of a direct transsylvian approach, and exposes the target in a wide working angle within a short distance. Despite some limitations in exposure, SOKC is suitable for a direct subfrontal approach, and provides a more anteromedial and basal view. MCAB and posteriorly directing ICA terminal aneurysms can be good candidates for MPKC.
Keyword
MeSH Terms
Figure
-

Fig. 1 The illustration depicts the microscopically operable working angles for the anterior communicating artery, the terminal of the internal carotid artery, and the bifurcation of the middle cerebral artery when approached by the mini-pterional keyhole craniotomy (A) and the supraorbital keyhole craniotomy (B). The simplified diagram (C) describes the working angle (black arrow) and the trajectory line (asterisk). The working depth refers to the length of the trajectory line. The black arrow head indicates a half angle of the working angle.
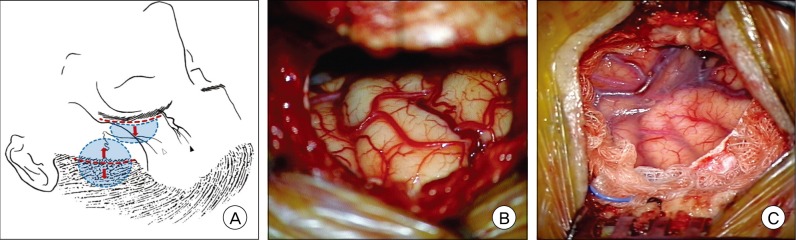
Fig. 2 The illustration (A) shows the different locations of the skin incision (red dotted line), size and shape of the bone flap (blue dotted line and area), and direction of skin retraction (red arrows) for the supraorbital keyhole craniotomy (SOKC) and the mini-pterional keyhole craniotomy (MPKC). The courses of the supraorbital nerve and artery (black arrow head) and the frontal branches of the facial nerve (white arrow head) are shown. Intraoperative photographs show the area of surgical exposure created by the SOKC (B) and MPKC (C). Note that the basal frontal lobe is exposed by the semilunar SOKC using only upward skin retraction, whereas the sylvian fissure is directly exposed by the MPKC using bilateral skin retraction.
Cited by 2 articles
-
A Simple Method for Reconstruction of the Temporalis Muscle Using Contourable Strut Plate after Pterional Craniotomy: Introduction of the Surgical Techniques and Analysis of Its Efficacy
Jin-Hack Park, Yoon-Soo Lee, Sang-Jun Suh, Jeong-Ho Lee, Kee-Young Ryu, Dong-Gee Kang
J Cerebrovasc Endovasc Neurosurg. 2015;17(2):93-100. doi: 10.7461/jcen.2015.17.2.93.Keyhole approach in anterior circulation aneurysm: Current indication, advantages, technical limitations, complications and their avoidance
Hanuman Prajapati, Ahmad Ansari, Manish Jaiswal
J Cerebrovasc Endovasc Neurosurg. 2022;24(2):101-112. doi: 10.7461/jcen.2022.E2021.07.008.
Reference
-
1. Andaluz N, Romano A, Reddy LV, Zuccarello M. Eyelid approach to the anterior cranial base. J Neurosurg. 2008; 8. 109(2):341–346. PMID: 18671651.
Article2. Badie B. Cosmetic reconstruction of temporal defect following pterional [corrected] craniotomy. Surg Neurol. 1996; 4. 45(4):383–384. PMID: 8607091.3. Chalouhi N, Jabbour P, Ibrahim I, Starke RM, Younes P, El Hage G, et al. Surgical treatment of ruptured anterior circulation aneurysms: comparison of pterional and supraorbital keyhole approaches. Neurosurgery. 2013; 3. 72(3):437–442. PMID: 23208062.4. Coscarella E, Vishteh AG, Spetzler RF, Seoane E, Zabramski JM. Subfascial and submuscular methods of temporal muscle dissection and their relationship to the frontal branch of the facial nerve. Technical note. J Neurosurg. 2000; 5. 92(5):877–880. PMID: 10794306.5. Dare AO, Landi MK, Lopes DK, Grand W. Eyebrow incision for combined orbital osteotomy and supraorbital minicraniotomy: application to aneurysms of the anterior circulation. Technical note. J Neurosurg. 2001; 10. 95(4):714–718. PMID: 11596969.6. Figueiredo EG, Deshmukh P, Nakaji P, Crusius MU, Crawford N, Spetzler RF, et al. The minipterional craniotomy: technical description and anatomic assessment. Neurosurgery. 2007; 11. 61(5 Suppl 2):256–264. discussion 264-5. PMID: 18091240.
Article7. Jallo GI, Suk I, Bognár L. A superciliary approach for anterior cranial fossa lesions in children. Technical note. J Neurosurg. 2005; 7. 103(1 Suppl):88–93. PMID: 16122012.8. Kil JS, Kim DW, Kang SD. Navigation-guided keyhole approach for unruptured intracranial aneurysms. Korean J Cerebrovasc Surg. 2011; 9. 13(3):244–248.9. Lee MS, Lee YS, Lee JH, Ryu KY, Kang DG. The efficacy of temporal mesh plate floating technique for keyhole site depression after frontotemporal craniotomy. J Korean Neurotraumatol Soc. 2011; 7:78–82.
Article10. Nathal E, Gomez-Amador JL. Anatomic and surgical basis of the sphenoid ridge keyhole approach for cerebral aneurysms. Neurosurgery. 2005; 1. 56(1 Suppl):178–185. discussion 178-85. PMID: 15799808.
Article11. Park HS, Park SK, Han YM. Microsurgical experience with supraorbital keyhole operations on anterior circulation aneurysms. J Korean Neurosurg Soc. 2009; 8. 46(2):103–108. PMID: 19763211.
Article12. Reisch R, Perneczky A. Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery. 2005; 10. 57(4 Suppl):242–255. discussion 242-55. PMID: 16234671.
Article13. Renowden SA, Benes V, Bradley M, Molyneux AJ. Detachable coil embolisation of ruptured intracranial aneurysms: a single center study, a decade experience. Clin Neurol Neurosurg. 2009; 2. 111(2):179–188. PMID: 19013012.
Article14. Sánchez-Vázquez MA, Barrera-Calatayud P, Mejia-Villela M, Palma-Silva JF, Juan-Carachure I, Gomez-Aguilar JM, et al. Transciliary subfrontal craniotomy for anterior skull base lesions. Technical note. J Neurosurg. 1999; 11. 91(5):892–896. PMID: 10541254.15. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms: concept and technique. Surg Neurol. 1998; 5. 49(5):481–489. discussion 489-90. PMID: 9586924.
Article16. Yaşargil MG, Antic J, Laciga R, Jain KK, Hodosh RM, Smith RD. Microsurgical pterional approach to aneurysms of the basilar bifurcation. Surg Neurol. 1976; 8. 6(2):83–91. PMID: 951657.17. Yaşargil MG, Boehm WB, Ho RE. Microsurgical treatment of cerebral aneurysms at the bifurcation of the internal carotid artery. Acta Neurochir (Wien). 1978; 41(1-3):61–72. PMID: 665339.
Article18. Yaşargil MG, Fox JL. The microsurgical approach to intracranial aneurysms. Surg Neurol. 1975; 1. 3(1):7–14. PMID: 1111150.19. Yaşargil MG, Reichman MV, Kubik S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg. 1987; 9. 67(3):463–466. PMID: 3612281.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microsurgical Experience with Supraorbital Keyhole Operations on Anterior Circulation Aneurysms
- Comparison between Lateral Supraorbital Approach and Pterional Approach in the Surgical Treatment of Unruptured Intracranial Aneurysms
- Superciliary Keyhole Approach for Unruptured Anterior Circulation Aneurysms: Surgical Technique, Indications, and Contraindications
- Unruptured Supraclinoid Internal Carotid Artery Aneurysm Surgery : Superciliary Keyhole Approach versus Pterional Approach
- Keyhole Approach and Neuroendoscopy for Cerebral Aneurysms
