Ann Dermatol.
2011 Aug;23(3):348-351. 10.5021/ad.2011.23.3.348.
Successful Treatment of Cutaneous Lesions of Dermatomyositis with Topical Pimecrolimus
- Affiliations
-
- 1Department of Dermatology, Hanyang University Hospital, Hanyang University College of Medicine, Seoul, Korea. drko0303@hanyang.ac.kr
- KMID: 2171927
- DOI: http://doi.org/10.5021/ad.2011.23.3.348
Abstract
- Dermatomyositis (DM) is an idiopathic inflammatory process characterized by proximal muscle weakness and cutaneous lesions, such as the Gottron's sign, heliotrope rash, and erythematous photosensitive rash. Administration of systemic agents for the treatment of underlying systemic diseases leads to remission of the cutaneous lesions in many cases. However, cutaneous lesions may remain refractory to treatment. Pimecrolimus is a calcineurin inhibitor with combined anti-inflammatory and immunomodulatory activity. It has high affinity to the skin and low permeation potential, even in patients with acute skin inflammation and in those undergoing post-topical corticosteroid therapy. We herein report two DM patients whose cutaneous lesions were refractory to conventional treatment but showed dramatic response to topical pimecrolimus. The clinical outcomes suggest that topical pimecrolimus may be a good therapeutic alternative for the management of the cutaneous lesions of DM.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Patient 1 with the shawl sign before treatment. (B) Gottron's sign before treatment. (C, D) Two months later after treatment with topical pimecrolimus. (E, F) Ten months later after treatment with topical pimecrolimus.
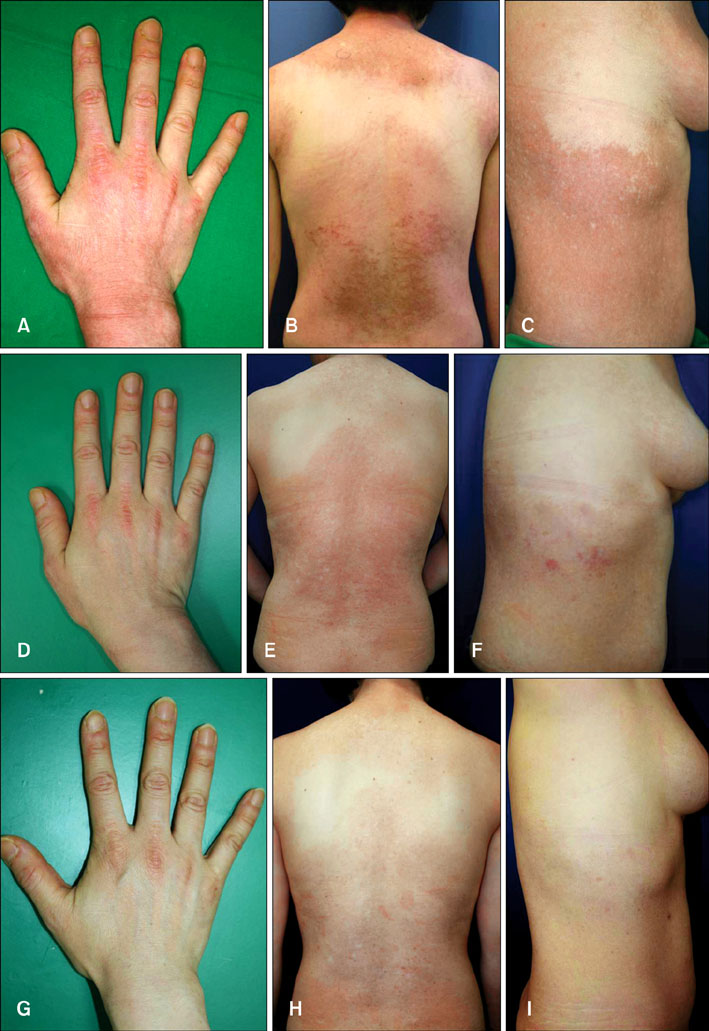
Fig. 2 (A) Patient 2 with the Gottron's sign before treatment. (B) Poikilodermatous erythematous patch on the nape and trunk before treatment. (C) Poikilodermatous erythematous patch on the right flank before treatment. (D, E, F) Three months after treatment with topical pimecrolimus. (G, H, I) One year later after stopping topical pimecrolimus treatment.
Reference
-
1. Kovacs SO, Kovacs SC. Dermatomyositis. J Am Acad Dermatol. 1998. 39:899–920.
Article2. Dawkins MA, Jorizzo JL, Walker FO, Albertson D, Sinal SH, Hinds A. Dermatomyositis: a dermatology-based case series. J Am Acad Dermatol. 1998. 38:397–404.
Article3. Gupta AK, Chow M. Pimecrolimus: a review. J Eur Acad Dermatol Venereol. 2003. 17:493–503.
Article4. Sontheimer RD, Costner MI. Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Dermatomyositis. Fitzpatrick's dermatology in general medicine. 2008. 7th ed. New York: McGraw-Hill;1536–1553.5. Ho S, Clipstone N, Timmermann L, Northrop J, Graef I, Fiorentino D, et al. The mechanism of action of cyclosporin A and FK506. Clin Immunol Immunopathol. 1996. 80:S40–S45.
Article6. Hoetzenecker W, Meingassner JG, Ecker R, Stingl G, Stuetz A, Elbe-Bürger A. Corticosteroids but not pimecrolimus affect viability, maturation and immune function of murine epidermal Langerhans cells. J Invest Dermatol. 2004. 122:673–684.
Article7. Meingassner JG, Aschauer H, Stuetz A, Billich A. Pimecrolimus permeates less than tacrolimus through normal, inflamed, or corticosteroid-pretreated skin. Exp Dermatol. 2005. 14:752–757.
Article8. Rodríguez-Martín M, Sáez-Rodríguez M, Carnerero-Rodríguez A, Rodríguez-García F, Cabrera de Paz R, Sidro-Sarto M, et al. Treatment of perioral dermatitis with topical pimecrolimus. J Am Acad Dermatol. 2007. 56:529–530.
Article9. Tzellos TG, Kouvelas D. Topical tacrolimus and pimecrolimus in the treatment of cutaneous lupus erythematosus: an evidence-based evaluation. Eur J Clin Pharmacol. 2008. 64:337–341.
Article10. Lampropoulos CE, D' Cruz DP. Topical tacrolimus treatment in a patient with dermatomyositis. Ann Rheum Dis. 2005. 64:1376–1377.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Four Cases of Facial Discoid Lupus Erythematosus Successfully Treated with Topical Pimecrolimus or Tacrolimus
- A Case of Generalized Lichen Planus Treated with Topical Pimecrolimus
- Lichen Striatus in a Girl: Successful Treatment with Pimecrolimus
- A Case of Tinea Incognito Induced by 1% Pimecrolimus (Elidel(R)) Cream
- A Case of Amyopathic Dermatomyositis
