Late-onset Systemic Lupus Erythematosus with Protein-losing Enteropathy, Vitiligo, and Diffuse Alveolar Hemorrhage
- Affiliations
-
- 1Department of General Medicine, JCHO Hokkaido Hospital, Sapporo, Japan. masshi@isis.ocn.ne.jp
- 2Department of Nephrology, JCHO Hokkaido Hospital, Sapporo, Japan.
- 3Department of Dermatology, JCHO Hokkaido Hospital, Sapporo, Japan.
- KMID: 2171349
- DOI: http://doi.org/10.12771/emj.2015.38.3.121
Abstract
- A 60-year-old man who had been diagnosed with protein-losing enteropathy (PLE) and vitiligo at age 51 years was admitted with dyspnea, hemoptysis, and lower-limb edema. On the basis of computed tomography findings, the cause of respiratory symptoms was thought to be diffuse alveolar hemorrhage (DAH). The final diagnosis of late-onset systemic lupus erythematosus (SLE) was established on the basis of renal biopsy examinations that revealed evidence of active SLE with lupus nephritis (World Health Organization, class V) and positive results for antinuclear antibody. DAH, as well as PLE and vitiligo were attributed to SLE. The patient was successfully treated with methylprednisolone and then prednisolone in combination with cyclosporin A. Because late-onset SLE is rare and patients tend to show atypical symptoms, close attention should be paid to the preceding symptoms.
MeSH Terms
Figure
-

Fig. 1 Vitiligo. Depigmented patches are shown on the neck and upper back (A) and on the arm (B).
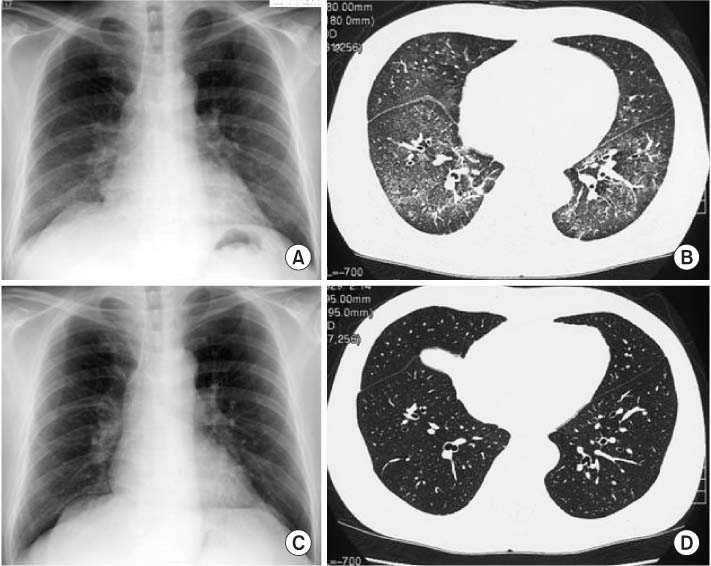
Fig. 2 Radiologic findings at initial presentation (A, B) and after treatment (C, D).(A) A chest radiograph shows bilateral, slightly reticular opacities predominantly in the middle and lower lung fields. (B) A high-resolution chest computed tomography (CT) shows bilateral ground-glass opacities, with relative sparing of the peripheral lung parenchyma. (C) A chest radiograph shows no abnormal findings. (D) A high-resolution chest CT shows no abnormal findings.
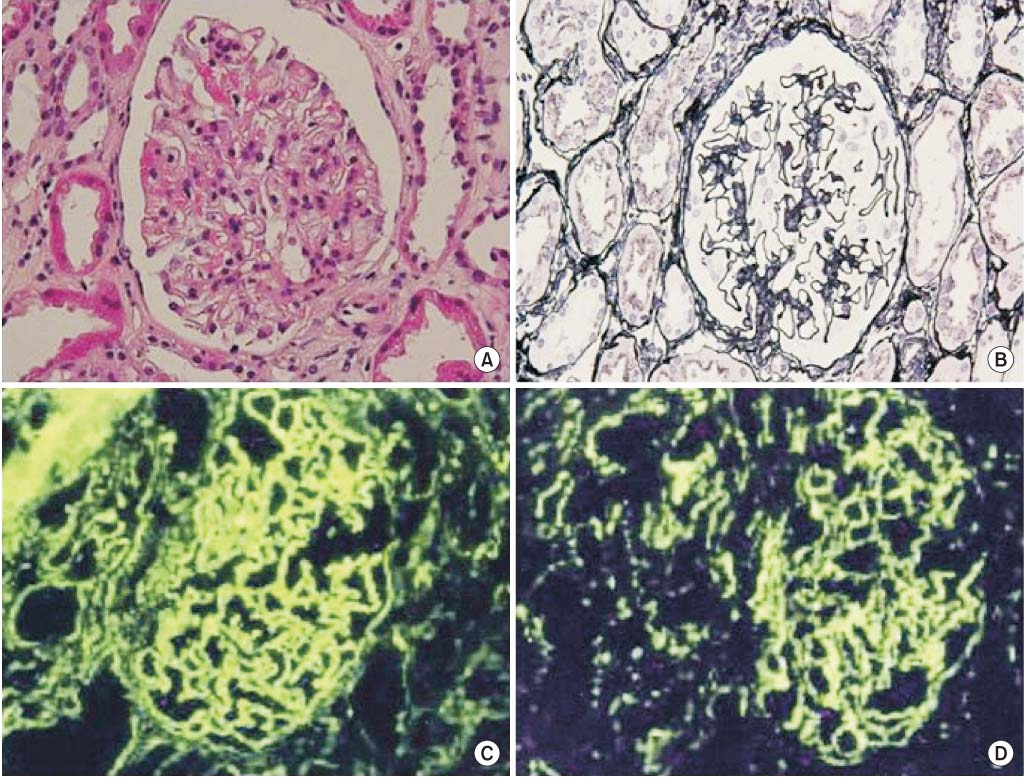
Fig. 3 Histologic findings. (A) Light microscopy of a renal biopsy specimen shows no significant glomerular findings (H&E, ×400). (B) Periodic acid methenamine silver staining shows spike formation in the basement membrane (×400). (C) Immunofluorescence microscopy shows diffuse granular deposits of IgG in the basement membrane (×400). (D) Immunofluorescence microscopy shows diffuse granular deposits of C3 in the basement membrane (×400).
Reference
-
1. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997; 40:1725.2. Petri M, Orbai AM, Alarcon GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012; 64:2677–2686.3. Matsumoto M, Kaieda S, Honda S, Ida H, Hoshino T, Fukuda T. A case of late-onset systemic lupus erythematosus with severe anemia. Kurume Med J. 2013; 60:25–28.4. Stefanidou S, Gerodimos C, Benos A, Galanopoulou V, Chatziyannis I, Kanakoudi F, et al. Clinical expression and course in patients with late onset systemic lupus erythematosus. Hippokratia. 2013; 17:153–156.5. Rovensky J, Tuchynova A. Systemic lupus erythematosus in the elderly. Autoimmun Rev. 2008; 7:235–239.6. Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P, et al. Systemic lupus erythematosus: clinical and immunologic patterns of disease expression in a cohort of 1,000 patients. The European Working Party on Systemic Lupus Erythematosus. Medicine (Baltimore). 1993; 72:113–124.7. Maddison P, Farewell V, Isenberg D, Aranow C, Bae SC, Barr S, et al. The rate and pattern of organ damage in late onset systemic lupus erythematosus. J Rheumatol. 2002; 29:913–917.8. Mak SK, Lam EK, Wong AK. Clinical profile of patients with lateonset SLE: not a benign subgroup. Lupus. 1998; 7:23–28.9. Tomic-Lucic A, Petrovic R, Radak-Perovic M, Milovanovic D, Milovanovic J, Zivanovic S, et al. Late-onset systemic lupus erythematosus: clinical features, course, and prognosis. Clin Rheumatol. 2013; 32:1053–1058.10. Lalani S, Pope J, de Leon F, Peschken C. Members of CaNIOS/1000 Faces of Lupus. 1000 Faces of Lupus. Clinical features and prognosis of late-onset systemic lupus erythematosus: results from the 1000 faces of lupus study. J Rheumatol. 2010; 37:38–44.11. Chen TL, Wong CH, Lee CS, Loo JH, Lin M. Systemic lupus erythematosus in the elderly. Int J Gerontol. 2009; 3:108–113.12. Walsh DS, Farley MF, Beard JS, Sau P, Tesar J, James WD. Systemic lupus erythematosus: nephritis, dilated cardiomyopathy, and extensive cutaneous depigmentation responsive to hydroxychloroquine. J Am Acad Dermatol. 1995; 33(5 Pt 1):828–830.13. Archimandritis A, Tsirantonaki M, Tzivras M, Hatzis G, Davaris P. Watermelon stomach in a patient with vitiligo and systemic lupus erythematosus. Clin Exp Rheumatol. 1996; 14:227–228.14. Nath SK, Kelly JA, Namjou B, Lam T, Bruner GR, Scofield RH, et al. Evidence for a susceptibility gene, SLEV1, on chromosome 17p13 in families with vitiligo-related systemic lupus erythematosus. Am J Hum Genet. 2001; 69:1401–1406.15. Park MS. Diffuse alveolar hemorrhage. Tuberc Respir Dis (Seoul). 2013; 74:151–162.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of systemic lupus erythematosus with chylothorax, chronic interstitial cystitis and protein-losing enteropathy
- A Case of Protein-losing Enteropathy Treated with High Dose Intravenous Glucocorticoid Therapy in Systemic Lupus Erythematosus
- A Case of Protein Losing Enteropathy as Only Clinical manifestation of Systemic Lupus Erythematosus
- A Case of Annular Polycyclic Type of Subacute Cutaneous Lupus Erythematosus with Protein Losing Enteropathy
- A Systemic Lupus Erythematosus Patient with Protein Losing Enteropathy
