Pulmonary Tumor Thrombotic Microangiopathy Associated with Advanced Gastric Cancer Successfully Treated with Chemotherapy
- Affiliations
-
- 1Department of Internal Medicine, KEPCO Medical Center, Seoul, Korea. parkkoh@daum.net
- 2Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 3Laboratory Medicine, KEPCO Medical Center, Seoul, Korea.
- KMID: 2171300
- DOI: http://doi.org/10.12771/emj.2014.37.2.146
Abstract
- Pulmonary tumor thrombotic microangiopathy (PTTM) is an uncommon and fatal malignancy-related pulmonary complication characterized by fibrocellular intimal proliferation of small pulmonary arteries and arterioles. It causes marked pulmonary hypertension, right-side heart failure, and sudden death. Diagnosis of PTTM is extremely difficult while the patient is alive. Here, we report a 44-year-old woman who presented with complaining of progressing dyspnea and pulmonary hypertension but with no history of cancer. She was diagnosed with PTTM caused by advanced gastric cancer ante mortem and was treated effectively with chemotherapy.
Keyword
MeSH Terms
Figure
-
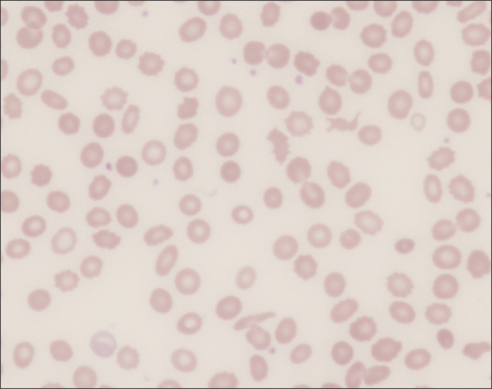
Fig. 1 Peripheral blood smear. It shows schistocytes and reticulocytes, consistent with microangiopathic hemolytic anemia (×400).

Fig. 2 Pulmonary computed tomography angiogram. It shows no abnormalities in the pulmonary artery, but enlargement of the right atrium and ventricle are observed (A). There are no significant abnormalities in the lung parenchyme (B).

Fig. 3 The echocardiogram. It shows typical findings of acute pulmonary thromboembolism with a D-shaped left ventricle, right ventricular enlargement without hypokinesia, moderate tricuspid regurgitation, and severe pulmonary hypertension with right ventricular systolic pressure of 79 mmHg.
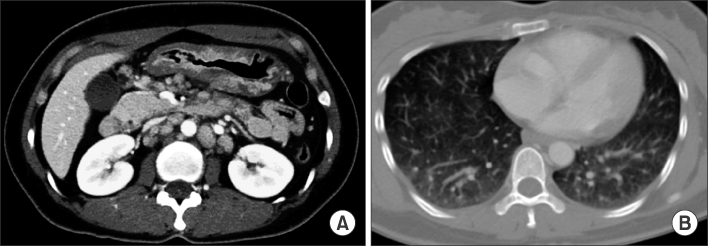
Fig. 4 Abdomino-pelvic computed tomography (CT). It shows diffusely thickened gastric antrum wall and multiple enlarged lymph nodes in celiac, paraaortic, aortocaval, and mesenteric lesions (A). In the lung parenchyme of the abdominopelvic CT, ground-glass opacities and reticulonodular infiltration with tree-in-bud form appeared compared with the initial pulmonary CT (B).

Fig. 5 Gastroduodenoscopic finding. (A) Gastroduodenoscopy shows an ulcerofungating mass with folds converging from the low body to the proximal antrum. (B) Microscopically, the stomach biopsy shows poorly differentiated adenocarcinoma (H&E, ×100). (C) Microscopically, the lymph node biopsy shows metastatic adenocarcinoma (H&E, ×100).
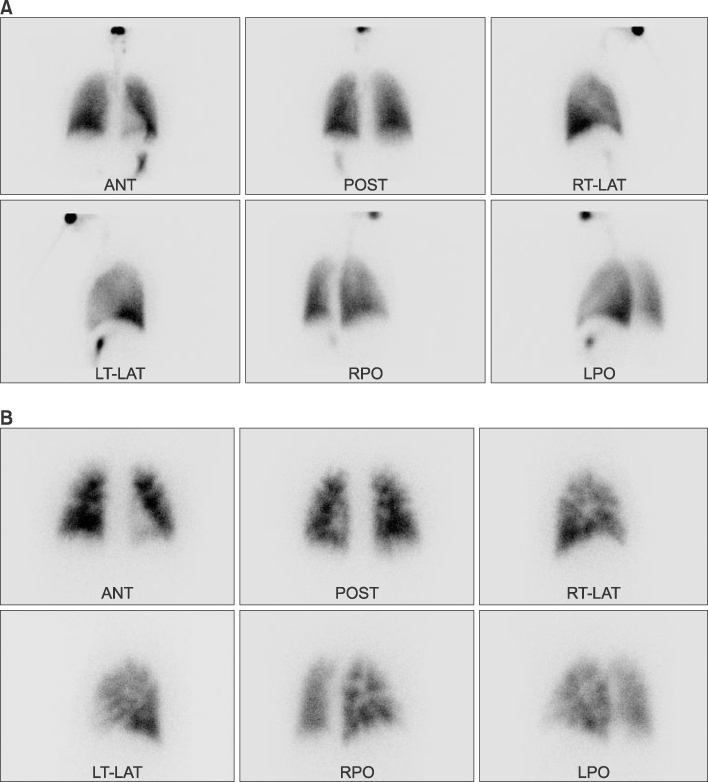
Fig. 6 Lung and perfusion scans. (A) Lung scan shows no defects in the lung ventilation. (B) The perfusion scan shows multiple small wedge-shaped perfusion defects throughout both lungs and the periphery. This finding is compatible with a tumor microembolism. ANT, anterior; POST, posterior; RT-LAT, right lateral; LT-LAT, left lateral; RPO, right posterior oblique; LPO, left posterior oblique.
Reference
-
1. von Herbay A, Illes A, Waldherr R, Otto HF. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer. 1990; 66:587–592.2. Sato Y, Marutsuka K, Asada Y, Yamada M, Setoguchi T, Sumiyoshi A. Pulmonary tumor thrombotic microangiopathy. Pathol Int. 1995; 45:436–440.3. Okubo Y, Wakayama M, Kitahara K, Nemoto T, Yokose T, Abe F, et al. Pulmonary tumor thrombotic microangiopathy induced by gastric carcinoma: morphometric and immunohistochemical analysis of six autopsy cases. Diagn Pathol. 2011; 6:27.4. Kim HJ, Kwak MH, Kong SY, Seong MW, Kang HS, Lee KS, et al. A case of locally advanced breast cancer complicated by pulmonary tumor thrombotic microangiopathy. Cancer Res Treat. 2012; 44:267–270.5. Yoo JH, Kim YH, Kim DY, Kang HY, Kim IJ, Lim SW, et al. Pulmonary tumor thrombotic microangiopathy in a patient with breast cancer. Korean J Med. 2009; 76:Suppl 1. S87–S92.6. Miyano S, Izumi S, Takeda Y, Tokuhara M, Mochizuki M, Matsubara O, et al. Pulmonary tumor thrombotic microangiopathy. J Clin Oncol. 2007; 25:597–599.7. Kayatani H, Matsuo K, Ueda Y, Matsushita M, Fujiwara K, Yonei T, et al. Pulmonary tumor thrombotic microangiopathy diagnosed antemortem and treated with combination chemotherapy. Intern Med. 2012; 51:2767–2770.8. Kitamura A, Nishimura N, Jinta T, Suda R, Yamano Y, Ishikawa G, et al. A case of pulmonary tumor thrombotic microangiopathy diagnosed by transbronchial lung biopsy and treated with chemotherapy and long-term oxygen and anticoagulation therapies. Case Rep Pulmonol. 2013; 2013:259080.9. Chinen K, Tokuda Y, Fujiwara M, Fujioka Y. Pulmonary tumor thrombotic microangiopathy in patients with gastric carcinoma: an analysis of 6 autopsy cases and review of the literature. Pathol Res Pract. 2010; 206:682–689.10. Franquet T, Gimenez A, Prats R, Rodriguez-Arias JM, Rodriguez C. Thrombotic microangiopathy of pulmonary tumors: a vascular cause of tree-in-bud pattern on CT. AJR Am J Roentgenol. 2002; 179:897–899.11. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 19-1995. A 55 year-old woman with acute respiratory failure and radiographically clear lungs. N Engl J Med. 1995; 332:1700–1707.12. Fisher DC, Sherrill GB, Hussein A, Rubin P, Vredenburgh JJ, Elkordy M, et al. Thrombotic microangiopathy as a complication of high-dose chemotherapy for breast cancer. Bone Marrow Transplant. 1996; 18:193–198.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Locally Advanced Breast Cancer Complicated by Pulmonary Tumor Thrombotic Microangiopathy
- Fatal progressive right heart failure in a pancreatic cancer patient
- A Case of Pulmonary Tumor Thrombotic Microangiopathy in a Patient with Advanced Gastric Cancer
- A Case Report: Cavitary Infarction Caused by Pulmonary Tumor Thrombotic Microangiopathy in a Patient with Pancreatic Intraductal Papillary Mucinous Neoplasm
- Occult Gastric Cancer Presenting as Hypoxia from Pulmonary Tumor Thrombotic Microangiopathy
