Co-Occurrence of Papillary Thyroid Carcinoma and Mucosa-Associated Lymphoid Tissue Lymphoma in a Patient with Long-Standing Hashimoto Thyroiditis
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea. pons71@hanmail.net
- 2Biomedical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea.
- 3I Sam Internal Medicine Clinic, Busan, Korea.
- KMID: 2169314
- DOI: http://doi.org/10.3803/EnM.2013.28.4.341
Abstract
- Papillary thyroid carcinoma (PTC) is a common affliction of the thyroid gland, accounting for 70% to 80% of all thyroid cancers, whereas mucosa-associated lymphoid tissue (MALT) lymphoma of the thyroid gland is uncommon. The simultaneous occurrence of both malignancies is extremely rare. We report the case of a patient with both PTC and MALT lymphoma in the setting of Hashimoto thyroiditis. An 81-year-old female patient was first admitted with goiter and hoarseness, which was attributed to an ultrasonographic thyroid nodule. Subsequent fine-needle aspirate, interpreted as suspicious of papillary thyroid cancer, prompted total thyroidectomy. MALT lymphoma was an incidental postsurgical finding, coexisting with PTC in the setting of Hashimoto thyroiditis. Although the development of MALT lymphoma is very rare, patients with longstanding Hashimoto thyroiditis should undergo careful surveillance for both malignancies.
MeSH Terms
Figure
-
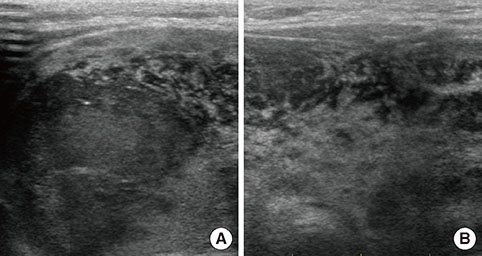
Fig. 1 (A) Thyroid ultrasonography shows an ill-defined hypoechogenic mass measuring 3.7×3.0 cm with microcalcifications in the right thyroid gland. (B) Left thyroid gland and isthmus show diffuse goiter with ill-defined multiple patchy hypoechogenicities and a heterogenicity.

Fig. 2 (A) Precontrast axial computed tomography (CT) scan shows a low density nodule (arrow) in the upper portion of the right thyroid gland. (B) Contrast-enhanced coronal CT scan shows a large, inhomogeneous enhancement of the left thyroid gland, displacing the trachea to the right, and a hyperintense nodule in the upper portion of the right thyroid gland (arrow).
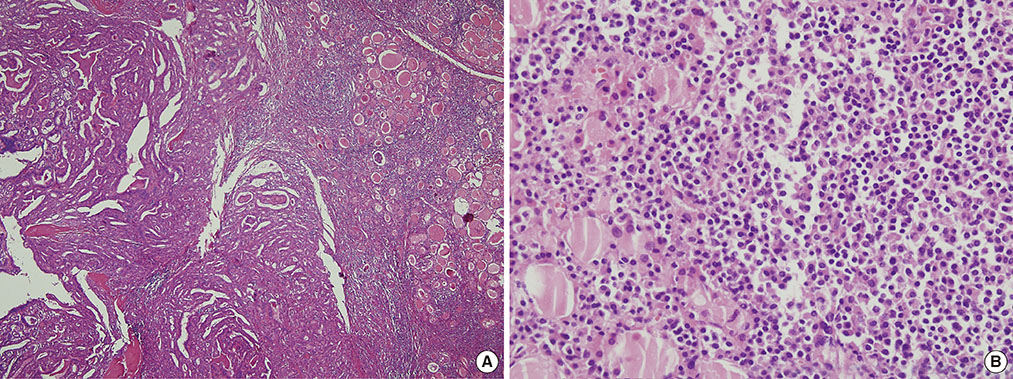
Fig. 3 (A) Histologic section of papillary thyroid carcinoma (left) and Hashimoto thyroiditis background (right) (H&E stain, ×40). (B) Hashimoto thyroiditis showing effacement of thyroid architecture by diffuse lymphocyte infiltration and residual thyroid follicles (H&E stain, ×400).
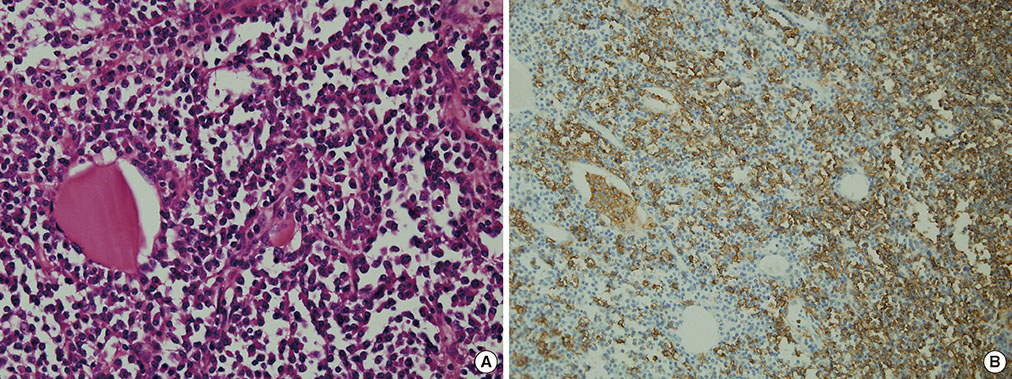
Fig. 4 (A) Effacement of thyroid architecture by neoplastic lymphoid infiltrate (H&E stain, ×400). (B) CD20-positive immunostaining of atypical small B cells (immunohistochemistry, ×200).
Cited by 2 articles
-
Brief Review of Articles in '
Endocrinology and Metabolism ' in 2013
Won-Young Lee
Endocrinol Metab. 2014;29(3):251-256. doi: 10.3803/EnM.2014.29.3.251.Synchronous Occurrence of Papillary Thyroid Carcinoma and Mucosa-Associated Lymphoid Tissue Lymphoma: a Single Case Report
Jun Suk Byun, Hye Yoon Lee, Ki Won Chun, Dae Sung Yoon
Int J Thyroidol. 2016;9(2):195-199. doi: 10.11106/ijt.2016.9.2.195.
Reference
-
1. Busnardo B, De Vido D. The epidemiology and etiology of differentiated thyroid carcinoma. Biomed Pharmacother. 2000; 54:322–326.2. Hakala T, Kellokumpu-Lehtinen P, Kholova I, Holli K, Huhtala H, Sand J. Rising incidence of small size papillary thyroid cancers with no change in disease-specific survival in finnish thyroid cancer patients. Scand J Surg. 2012; 101:301–306.3. Hwang YC, Kim TY, Kim WB, Shong YK, Yi KH, Shong M, Jo YS, Kim WS, Chung JH. Clinical characteristics of primary thyroid lymphoma in Koreans. Endocr J. 2009; 56:399–405.4. Derringer GA, Thompson LD, Frommelt RA, Bijwaard KE, Heffess CS, Abbondanzo SL. Malignant lymphoma of the thyroid gland: a clinicopathologic study of 108 cases. Am J Surg Pathol. 2000; 24:623–639.5. Holm LE, Blomgren H, Lowhagen T. Cancer risks in patients with chronic lymphocytic thyroiditis. N Engl J Med. 1985; 312:601–604.6. Cheng V, Brainard J, Nasr C. Co-occurrence of papillary thyroid carcinoma and primary lymphoma of the thyroid in a patient with long-standing Hashimoto's thyroiditis. Thyroid. 2012; 22:647–650.7. Melo GM, Sguilar DA, Petiti CM, Eichstaedt AG, Caiado RR, Souza RA. Concomitant thyroid Malt lymphoma and papillary thyroid carcinoma. Arq Bras Endocrinol Metabol. 2010; 54:425–428.8. Mack LA, Pasieka JL. An evidence-based approach to the treatment of thyroid lymphoma. World J Surg. 2007; 31:978–986.9. Thieblemont C, Mayer A, Dumontet C, Barbier Y, Callet-Bauchu E, Felman P, Berger F, Ducottet X, Martin C, Salles G, Orgiazzi J, Coiffier B. Primary thyroid lymphoma is a heterogeneous disease. J Clin Endocrinol Metab. 2002; 87:105–111.10. Tsang RW, Gospodarowicz MK, Pintilie M, Wells W, Hodgson DC, Sun A, Crump M, Patterson BJ. Localized mucosa-associated lymphoid tissue lymphoma treated with radiation therapy has excellent clinical outcome. J Clin Oncol. 2003; 21:4157–4164.11. Kini SR. Thyroid cytopathology: an atlas and text. 1st ed. Philadelphia: Lippincott Williams & Wilkins;2008. p. 322–326.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Synchronous Occurrence of Papillary Thyroid Carcinoma and Mucosa-Associated Lymphoid Tissue Lymphoma: a Single Case Report
- Ultrasonographic Findings of Papillary Thyroid Cancer with or without Hashimoto's Thyroiditis
- Primary Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma of Thyroid Gland Arising from Coexisting Hashimoto's Thyroiditis: A Case Report
- Thyroid MALT Lymphoma Associated with Thyroid Papillary Cancer
- Lymphocyte Rich Papillary Oxyphilic Carcinoma of Thyroid
