A Case of Pheochromocytoma Crisis with Acute Myocardial Infarction Induced by Glucocorticoids Administration
- Affiliations
-
- 1Department of Internal Medicine, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. jhnoh@paik.ac.kr
- 2Department of Pathology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- KMID: 2169071
- DOI: http://doi.org/10.3803/EnM.2010.25.3.240
Abstract
- The most common symptoms of pheochromocytoma are paroxysmal or sustained hypertension, or symptoms of paroxysmal adrenergic stimulation such as palpitation, headache, and diaphoresis. These patients can on rare occasion reveal or be complicated with cardiovascular symptoms such as arrhythmia, cardiomyopathy, acute coronary syndrome and cardiogenic shock. These cardiac manifestations of pheochromocytoma may delay the diagnosis, which can cause a catastrophic outcome. A pheochromocytoma crisis is provoked by surgery, anesthesia, exercise and, several drugs and it is known to be an endocrine emergency with mortality as high as 85%. Many classes of drugs are well known to precipitate adverse reactions, but the presentation of pheochromocytoma after the administration of steroid has rarely been reported. We report here on a case of pheochromocytoma crisis with acute myocardial infarction after the patient took prednisolone. Furthermore, we discuss the mechanism of glucocorticoid induced crisis and myocardial infarction in pheochromocytoma patients.
MeSH Terms
Figure
-
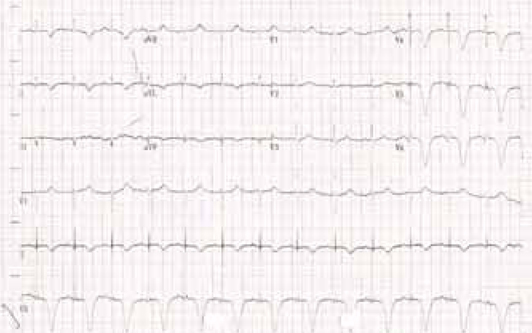
Fig. 1 Initial ECG at emergency room showed T wave inversion in precordial leads.
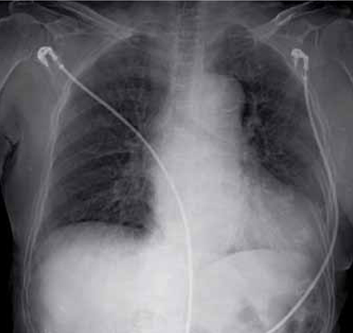
Fig. 2 Chest PA at admission reveals cardiomegaly, but no significant edema or active infiltrate.
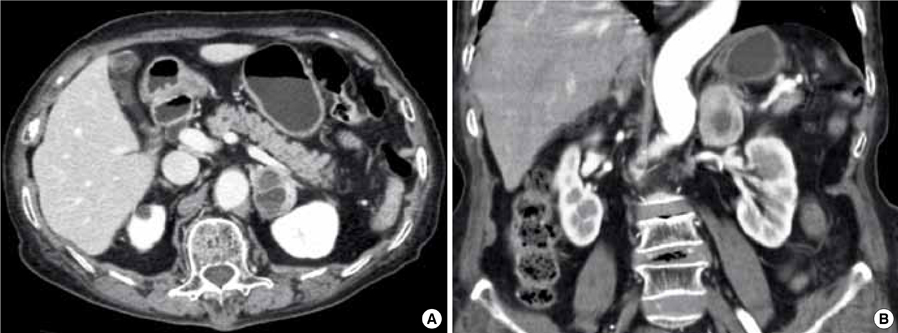
Fig. 3 Abdominal CT cross-section (A) and sagittal section (B) show 3.1 × 3.7 cm sized well-defined round ovoid shape mass with suspected necrosis or cystic change.

Fig. 4 A. Gross findings of the surgical specimen. The tumor is well demarcated with tan surface and central degeneration. Residual attached adrenal gland is present. B-D. Microscopic examination of the specimen. Organoid clusters of tumor cells are noted. The tumor cells have lavendar cytoplasm with punctate granularity (B, H&E, × 200). The tumor shows positive immunostaining for chromogranin (C, immunohistochemistry, × 200). Cells positive for S-100 protein are angular to stellate and are located at the periphery of alveolar clusters of tumor cells. These cells represent sustentacular cells (D, immunohistochemistry, × 100).
Reference
-
1. Young WF Jr. Kronrnberg HM, editor. Pheochromocytoma and paraganglioma. Williams textbook of endocrinology. 2008. 11th ed. Philadelphia: Saunders;507–522.2. Ahn YB, Kang MI, Lee KW, Son HY, Kang SK, Cha BY, Seo BJ, Jang KY, Yoon IJ, Lee SJ, Park SS, Oh YS. A case of pheochromocytoma with acute myocardial infarction. J Korean Endocr Soc. 1997. 12:655–660.3. Do MY, Kim HM, Ko YG, Lim SK, Jung JH, Chung N, Kim YA, Kang SA, Moon JH, Lee JH, Choi ST. A case of pheochromocytoma presented with cardiogenic shock. J Korean Endocr Soc. 2005. 20:283–288.4. Kim DS, Kim KR, Yoon HJ, Lee HK, Ryu JC, Kim DI, Yang TH. Two cases of pheochromocytoma associated with acute myocardial infarction. Korean J Med. 1999. 57:357–363.5. Leite LR, Macedo PG, Santos SN, Quaglia L, Mesas CE, De Paola A. Life-threatening cardiac manifestations of pheochromocytoma. Case Report Med. 2010. 2010:976120.6. Brouwers FM, Lenders JW, Eisenhofer G, Pacak K. Pheochromocytoma as an endocrine emergency. Rev Endocr Metab Disord. 2003. 4:121–128.7. Rosas AL, Kasperlik-Zaluska AA, Papierska L, Bass BL, Pacak K, Eisenhofer G. Pheochromocytoma crisis induced by glucocorticoids: a report of four cases and review of the literature. Eur J Endocrinol. 2008. 158:423–429.8. Rashid-Farokhi F, Cheraghvandi A, Masjedi MR. Pheochromocytoma crisis due to glucocorticoid administration: a case report and review of the literature. Arch Iran Med. 2009. 12:190–194.9. Ehrhart-Bornstein M, Hinson JP, Bornstein SR, Scherbaum WA, Vinson GP. Intraadrenal interactions in the regulation of adrenocortical steroidogenesis. Endocr Rev. 1998. 19:101–143.10. Wurtman RJ. Control of epinephrine synthesis in the adrenal medulla by the adrenal cortex: hormonal specificity and dose-response characteristics. Endocrinology. 1966. 79:608–614.11. Manger WM, Gifford RW Jr. Clinical and experimental pheochromocytoma. 1996. 2nd ed. Cambridge: Blackwell Science;144.12. Tischler AS, Perlman RL, Morse GM, Sheard BE. Glucocorticoids increase catecholamine synthesis and storage in PC12 pheochromocytoma cell cultures. J Neurochem. 1983. 40:364–370.13. Brown JW, Fishman LM, Carballeira A. Studies of the neuronal transdifferentiation process in cultured human pheochromocytoma cells: effects of steroids with differing functional groups on catecholamine content and cell morphology. Steroids. 1998. 63:587–594.14. McMahon A, Sabban EL. Regulation of expression of dopamine beta-hydroxylase in PC12 cells by glucocorticoids and cyclic AMP analogues. J Neurochem. 1992. 59:2040–2047.15. Goodman R, Edgar D, Thoenen H, Wechsler W, Herschman H. Glucocorticoid induction of tyrosine hydroxylase in a continuous cell line of rat pheochromocytoma. J Cell Biol. 1978. 78:R1–R7.16. Critchley JA, Henderson CG, Moffat LE, Ungar A, Waite J, West CP. Proceedings: The release of catecholamines from perfused canine adrenal glands by corticosteroids. J Physiol. 1976. 254:30P–31P.17. Yang S, Zhang L. Glucocorticoids and vascular reactivity. Curr Vasc Pharmacol. 2004. 2:1–12.18. Kurland GS, Freedberg AS. The potentiating effect of ACTH and of cortisone of pressor response to intravenous infusion of L-nor-epinephrine. Proc Soc Exp Biol Med. 1951. 78:28–31.19. Gupta KK. Letter: Phaeochromocytoma and myocardial infarction. Lancet. 1975. 1:281–282.20. Seeley E, Williams GH. Heart disease: a textbook of cardiovascular medicine: The heart in endocrine disorders. 2001. 6th ed. New York: W.B. Saunders;2163–2165.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Recurrent Glucocorticoid-Induced Pheochromocytoma Crisisb during the Treatment of Urticaria
- A complicated case of myocardial infarction with nonobstructive coronary arteries with an underlying pheochromocytoma: a case report
- A Case of Pheochromocytoma Presented with Acute Myocardial Infarction
- Myocardial Infarction in a Patient with Myocardial Bridge and Pheochromocytoma: A case report
- A Case of Pheochromocytoma with Acute Myocardial Infarction
