Resected femoral anthropometry for design of the femoral component of the total knee prosthesis in a Korean population
- Affiliations
-
- 1Catholic Institute for Applied Anatomy ; Department of Anatomy, School of Medicine, The Catholic University of Korea, Seoul, Korea. hsh@catholic.ac.kr
- 2Monte Vista Christian School class of 2012, California, USA.
- 3Somang Orthopedic Clinic, Seoul, Korea.
- KMID: 2168880
- DOI: http://doi.org/10.5115/acb.2010.43.3.252
Abstract
- We measured the mediolateral (ML) and anteroposterior (AP) length, height and widths of the anterior, posterior and inferior section of the resected distal femurs using three dimensional computer tomographic measurements in 200 knees from 100 cadavers. We also calculated the aspect ratio (ML/AP) and compared the measured parameters with that of six conventionally used total knee femoral prostheses. We found that the average ML (70.2+/-5.5 mm) and AP (53.9+/-3.8 mm) dimensions from our study were lower than those reported from Western populations. The aspect ratio showed a progressive decline with an increasing antero-posterior dimension. All of the compared designs showed undersizing for the mediolateral dimension distally and for the widths of the resected medial and lateral posterior femoral condyles. But some of the compared designs showed oversizing for the height of the resected medial and lateral posterior femoral condyles. This study provides guidelines for designing a suitable femoral component for total knee prostheses that fit Asian populations.
MeSH Terms
Figure
-

Fig. 1 Schematic representation of the (A) resected distal femoral surface showing the mediolateral (ML) dimension, anteroposterior (AP) dimension and the clinical epicondylar axis. Anterior and posterior cuts were made parallel to the clinical epicondylar axis. (B) resected anterior femoral condyle surface showing the heights of the anterior medial (HAM) and lateral condyles (HAL), width of the anterior condyle (WA). (C) resected posterior femoral condyle surface showing the heights (HPM and HPL) and widths (WPM and WPL) of the posterior medial and lateral femoral condyles.
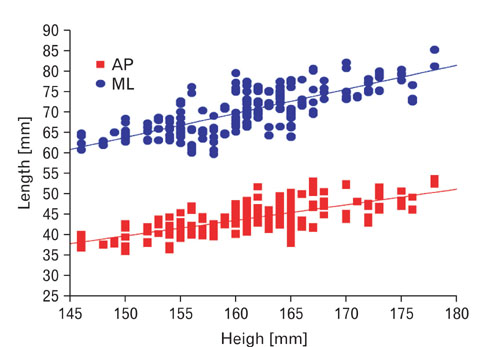
Fig. 2 Anteroposterior (AP) and mediolateral (ML) dimensions of the resected distal femoral compared to the height of the study population. Both AP and ML dimensions showed a positive correlation to the height of the population (r=0.7).
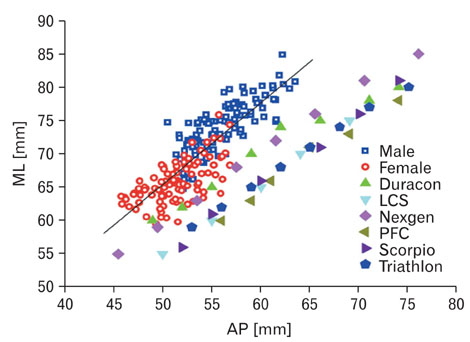
Fig. 3 The resected distal femoral mediolateral (ML) and anteroposterior (AP) dimensions in 100 knees of females and males each compared with that of the six conventional femoral designs of total knee arthroplasty. The lines represent the average values for the female and male population. All the femoral designs showed mediolateral undersizing for matching AP dimensions and no availability of smaller AP dimensions suited for our population.

Fig. 4 The distal femoral aspect ratio (ML/AP in %) and the anteroposterior dimension (AP) in 100 knees of females and males each compared with that of six conventional femoral designs. The line represents the average values for the female and male population. The population data shows a progressive decline in the aspect ratio with increasing size of the knee, whereas all of the femoral designs show a relatively constant aspect ratio.
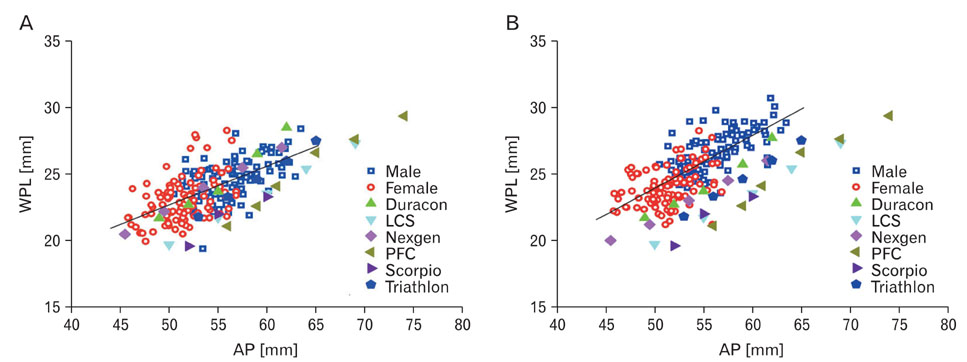
Fig. 5 Comparison of the width of the resected posterior femoral medial condyle (A) and posterior femoral lateral condyle (B) with that of femoral designs for matching AP dimensions. The line represents the average values for the female and male population. All designs show undercoverage for both condyles.
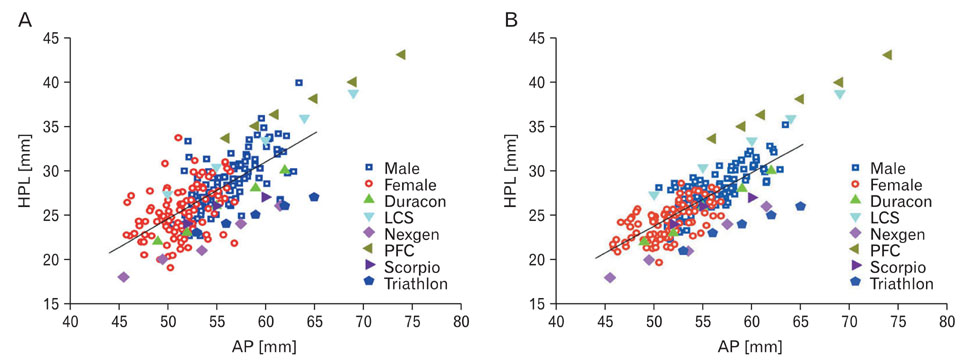
Fig. 6 Comparison of the height of the resected posterior femoral medial condyle (A) and posterior femoral lateral condyle (B) with that of the femoral designs for matching AP dimensions. The line represents the average values for the female and male population. The PFC femoral design closely matches our population data with larger AP dimensions.
Reference
-
1. Dorr LD, Boiardo RA. Technical considerations in total knee arthroplasty. Clin Orthop Relat Res. 1986. 205:5–11.2. Goldberg VM, Figgie HE 3rd, Figgie MP. Technical considerations in total knee surgery. Management of patella problems. Orthop Clin North Am. 1989. 20:189–199.3. Hitt K, Shurman JR 2nd, Greene K, et al. Anthropometric measurements of the human knee: correlation to the sizing of current knee arthroplasty systems. J Bone Joint Surg Am. 2003. 85-A:Suppl 4. 115–122.4. Ho WP, Cheng CK, Liau JJ. Morphometrical measurements of resected surface of femurs in Chinese knees: correlation to the sizing of current femoral implants. Knee. 2006. 13:12–14.5. Low FH, Khoo LP, Chua CK, Lo NN. Kinematic analysis of total knee prosthesis designed for Asian population. Crit Rev Biomed Eng. 2000. 28:33–40.6. Mensch JS, Amstutz HC. Knee morphology as a guide to knee replacement. Clin Orthop Relat Res. 1975. 112:231–241.7. Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am. 1987. 69:745–749.8. Ranawat CS. The patellofemoral joint in total condylar knee arthroplasty. Pros and cons based on five- to ten-year follow-up observations. Clin Orthop Relat Res. 1986. 205:93–99.9. Urabe K, Miura H, Kuwano T, et al. Comparison between the shape of resected femoral sections and femoral prostheses used in total knee arthroplasty in Japanese patients: simulation using three-dimensional computed tomography. J Knee Surg. 2003. 16:27–33.10. Vaidya SV, Ranawat CS, Aroojis A, Laud NS. Anthropometric measurements to design total knee prostheses for the Indian population. J Arthroplasty. 2000. 15:79–85.11. Wang SW, Feng CH, Lu HS. A study of Chinese knee joint geometry for prosthesis design. Chin Med J (Engl). 1992. 105:227–233.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fracture of the Femoral Component in Total Knee Arthroplasty Using Whiteside Ortholoc Prosthesis with Cement - Metallurgical Study by SEM and EDS
- Fracture of the Femoral Component in Whiteside Ortholoc Modular Total Knee ArthroplastyL: 2 Cases Reports
- Ultimate Determination of P.F.C Femoral Prosthetic size in TKR for the Elderly Patients
- The Study of Anatomical Measurement of Distal Femur and Compatibility of Femoral Prosthesis in Total Knee Arthroplasty
- The Discrepancy between Eipcondylar and Posterior Condylar Axis of Femur in Total Knee Arthroplasty
