Mechanical thrombectomy-assisted thrombolysis for acute symptomatic portal and superior mesenteric venous thrombosis
- Affiliations
-
- 1Department of Surgery, The Catholic University of Korea, Seoul St. Mary's Hospital, Seoul, Korea. vascularkim@catholic.ac.kr
- 2Department of Radiology, The Catholic University of Korea, Seoul St. Mary's Hospital, Seoul, Korea.
- 3Department of Surgery, Inha University Hospital, Inha University, Incheon, Korea.
- 4Department of Radiology, Inha University Hospital, Inha University, Incheon, Korea.
- KMID: 2167113
- DOI: http://doi.org/10.4174/astr.2014.86.6.334
Abstract
- Acute portal vein and mesenteric vein thrombosis (PVMVT) can cause acute mesenteric ischemia and be fatal with mortality rate of 37%-76%. Therefore, early diagnosis and prompt venous revascularization are warranted in patients with acute symptomatic PVMVT. Due to advances in catheter-directed treatment, endovascular treatment has been used for revascularization of affected vessels in PVMVT. We report two cases of symptomatic PVMVT treated successfully by transhepatic percutaneous mechanical thrombectomy-assisted thrombolysis.
MeSH Terms
Figure
-
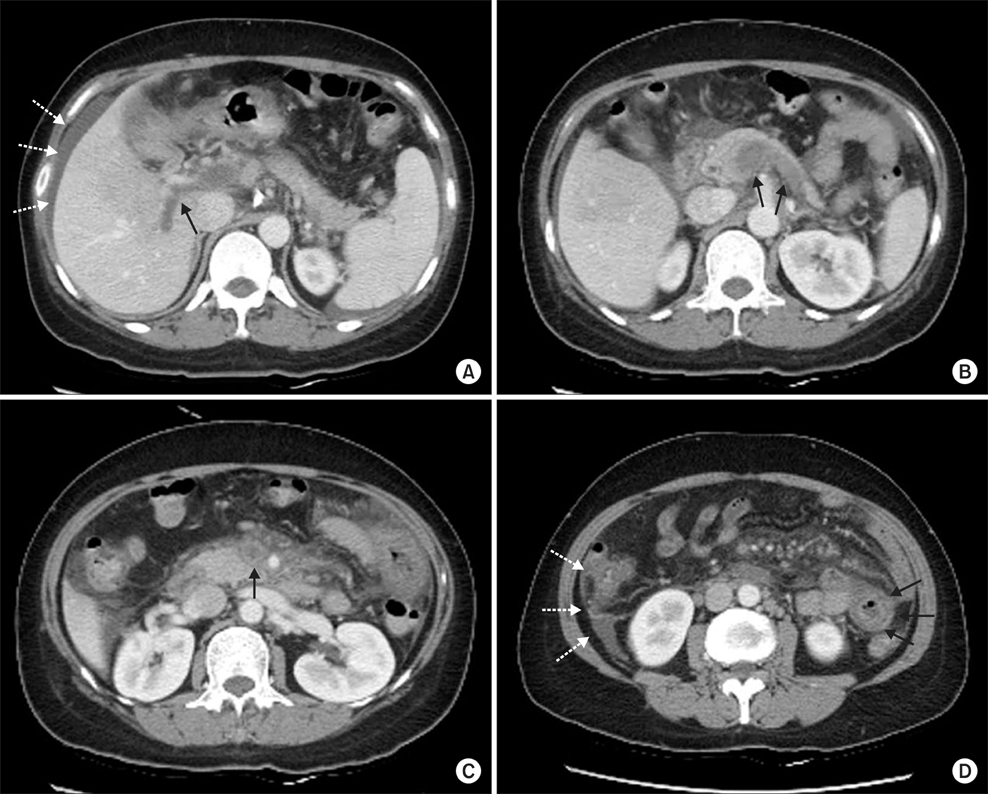
Fig. 1 Initial CT scan. Intraluminal thrombosis in the portal vein (A, arrow), splenic vein (B, arrows), and superior mesenteric vein (C, arrow) is evident. (D) Jejunal loop dilation and diffuse wall thickening (arrows) with a small amount of ascites are evident (dotted arrows; A, D).
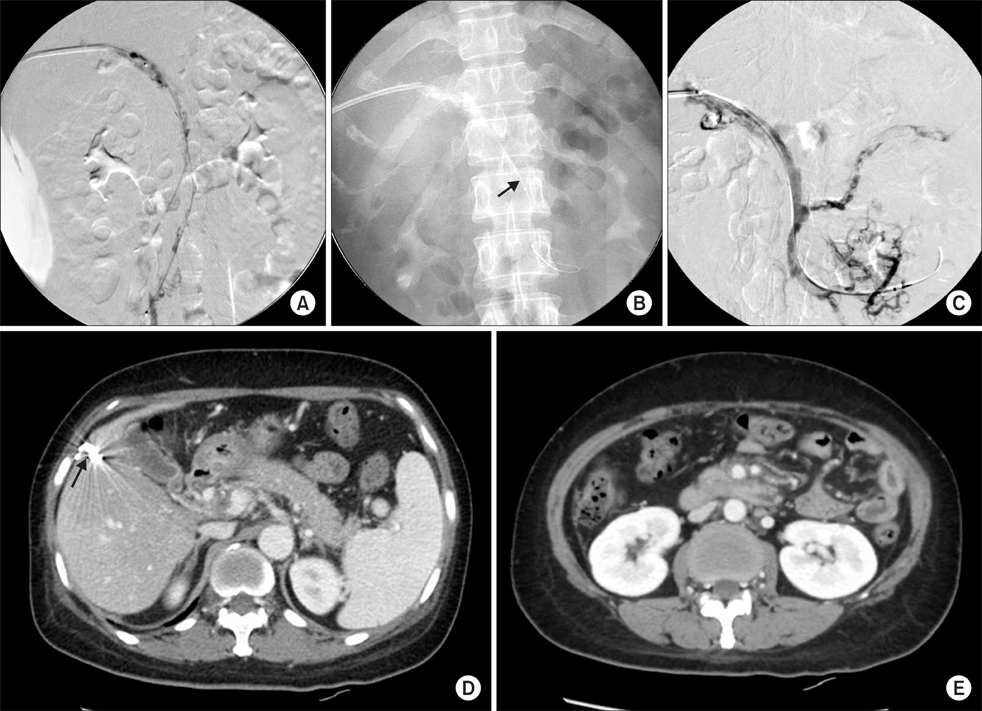
Fig. 2 (A) Portogram and mesenteric venogram showed extensive thrombosis in the portal vein and mesenteric vein. (B) AngioJet Spiroflex thrombectomy catheter in SMV (arrow). (C) The completion venogram demonstrated partial recanalization of venous flow in the portal vein and SMV and splenic vein. (D, E) Follow-up abdominal CT scan at the 16th hospital day. Improved blood flow with a small amount of residual intraluminal thrombus in the PV and SMV compared to the initial CT. (D) The puncture site of the liver was coil embolized (arrow). (E) Bowel loop dilatation and wall thickening also improved significantly.
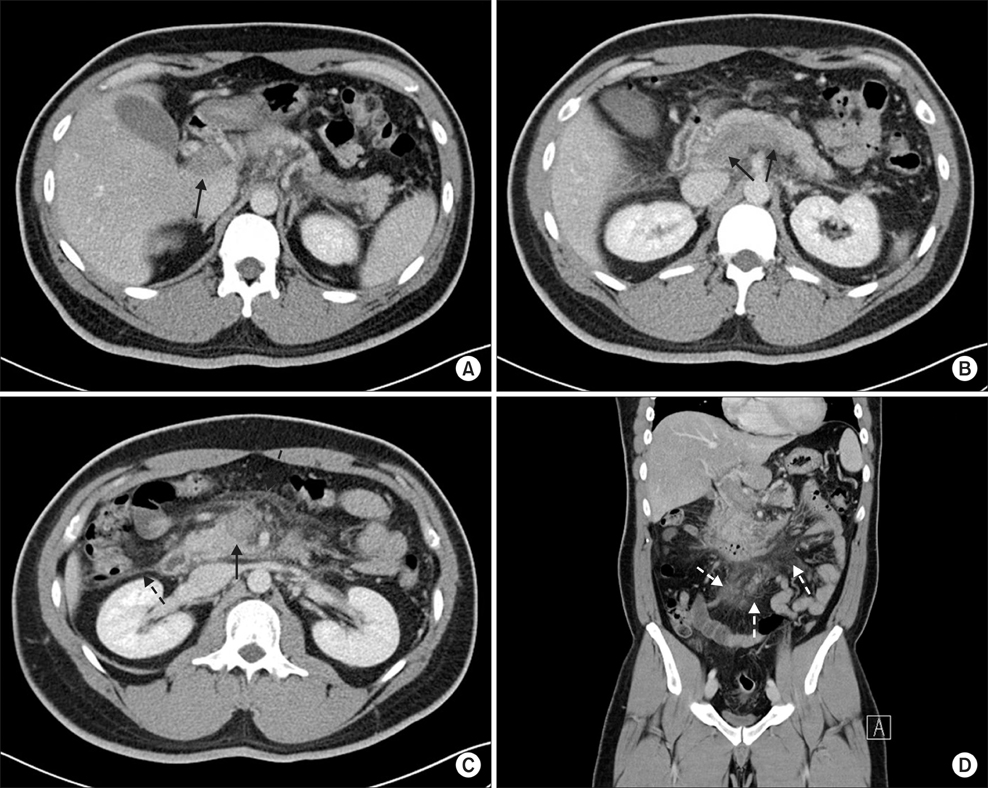
Fig. 3 Initial CT scan showed intraluminal thrombosis in the portal vein (A, arrow), splenic vein (B, arrows), and superior mesenteric vein (C, arrow). (C, D) Streaky infiltrations in the mesentery raised the suspicion of mesenteric edema (dotted arrows).
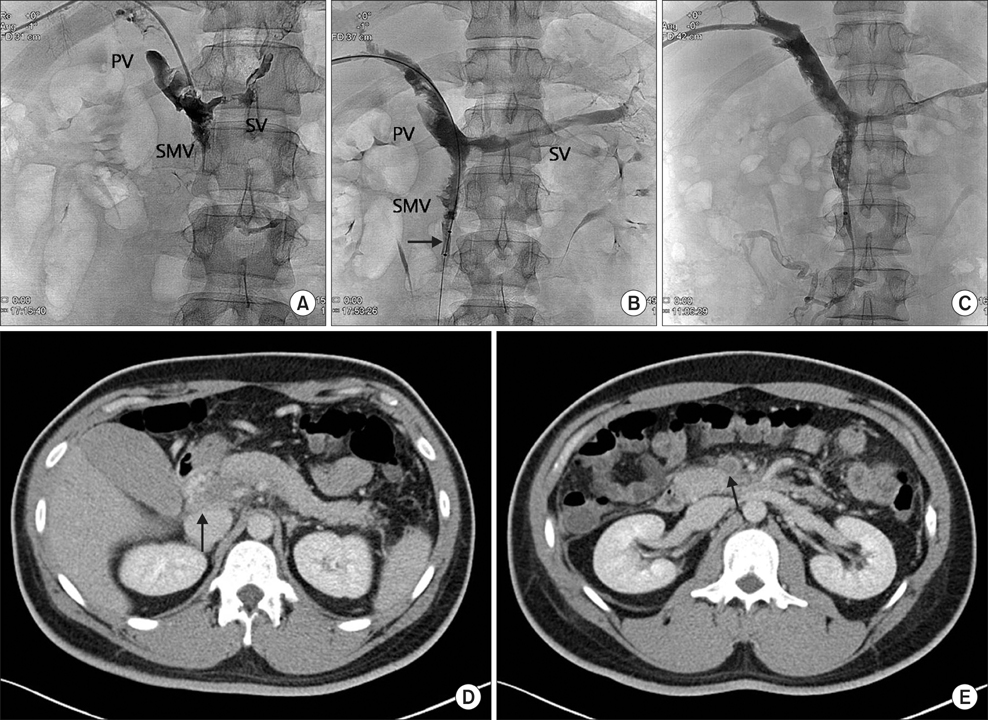
Fig. 4 (A) Venogram demonstrated extensive thrombosis in the portal vein (PV), superior mesenteric vein (SMV), and splenic vein (SV). (B) Using AngioJet catheter (arrow), mechanical thrombectomy was performed in the thrombosed segments of superior mesenteric vein. (C) Two days after the procedure, venography of superior mesenteric and portal veins demonstrated partial recanalization of these vessels. (D, E) Postprocedure 8th day abdominal CT scan. The volume of thrombi in the portal vein (D, arrow) and superior mesenteric vein (E, arrow) was decreased, and mesenteric edema had improved.

Fig. 5 Removed thrombi.
Reference
-
1. Chen C. Direct thrombolytic therapy in portal and mesenteric vein thrombosis. J Vasc Surg. 2012; 56:1124–1126.2. Lopera JE, Correa G, Brazzini A, Ustunsoz B, Patel S, Janchai A, et al. Percutaneous transhepatic treatment of symptomatic mesenteric venous thrombosis. J Vasc Surg. 2002; 36:1058–1061.3. Zhou W, Choi L, Lin PH, Dardik A, Eraso A, Lumsden AB. Percutaneous transhepatic thrombectomy and pharmacologic thrombolysis of mesenteric venous thrombosis. Vascular. 2007; 15:41–45.4. Kim HS, Patra A, Khan J, Arepally A, Streiff MB. Transhepatic catheter-directed thrombectomy and thrombolysis of acute superior mesenteric venous thrombosis. J Vasc Interv Radiol. 2005; 16:1685–1691.5. Uflacker R. Applications of percutaneous mechanical thrombectomy in transjugular intrahepatic portosystemic shunt and portal vein thrombosis. Tech Vasc Interv Radiol. 2003; 6:59–69.6. Rosen MP, Sheiman R. Transhepatic mechanical thrombectomy followed by infusion of TPA into the superior mesenteric artery to treat acute mesenteric vein thrombosis. J Vasc Interv Radiol. 2000; 11:195–198.7. Wissgott C, Kamusella P, Andresen R. Percutaneous mechanical thrombectomy: advantages and limitations. J Cardiovasc Surg (Torino). 2011; 52:477–484.8. Morgan R, Belli AM. Percutaneous thrombectomy: a review. Eur Radiol. 2002; 12:205–217.9. Sharafuddin MJ, Hicks ME. Current status of percutaneous mechanical thrombectomy. Part I. General principles. J Vasc Interv Radiol. 1997; 8:911–921.10. Sharafuddin MJ, Hicks ME. Current status of percutaneous mechanical thrombectomy. Part II. Devices and mechanisms of action. J Vasc Interv Radiol. 1998; 9:15–31.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combination of Surgical Thrombectomy and Direct Thrombolysis in Acute Abdomen with Portal and Superior Mesenteric Vein Thrombosis
- Acute Appendicitis with Superior Mesenteric Vein Thrombosis and Portal Vein Thrombosis
- Three cases of mesenteric venous thrombosis treated by different modalities
- Treatment of the Superior Sagittal Sinus Thrombosis with the Mechanical Thrombectomy Using Stent-Retriever Device
- Portal and Superior Mesenteric Venous Thrombosis Treated with Urokinase Infusion via Superior Mesenteric Artery
