Large cutaneous apocrine carcinoma occurring on right thigh aggravated after moxa treatment
- Affiliations
-
- 1Department of Pathology, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea.
- 2Department of Surgery, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea. ultravascsurg@gmail.com
- KMID: 2166999
- DOI: http://doi.org/10.4174/astr.2015.88.5.294
Abstract
- Primary cutaneous apocrine carcinoma is a rare adnexal tumor of the skin that occurs mainly in the axilla, anogenital area while the scalp and the lower extremities, especially the thigh, are very unusual sites. However, clinical or pathologic characteristics have not been well established due to a paucity of this tumor. Herein, we report very unusual case of apocrine carcinoma present as a huge mass in the lateral thigh of 77-year-old woman, which was aggravated abruptly after an irritation by moxa treatment, with a brief review of the literature.
MeSH Terms
Figure
-
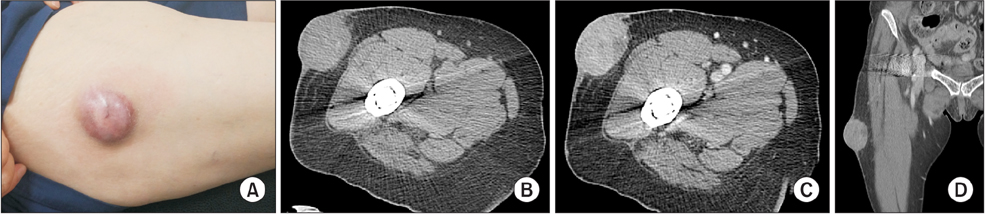
Fig. 1 (A) Grossly; large, firm, movable mass with thickened overlying skin is noted on anterolateral side of thigh, measuring about 6 cm in greatest dimension. (B) On precontrast CT, approximately 4.6 × 4.3-cm sized, oval shaped soft tissue mass is located in dermis and subcutis of right thigh having no connection with muscle. (C, D) After contrast injection, mass shows and heterogeneous enhancement and faint calcification.

Fig. 2 (A) At low power view, mass was relatively well defined but had focally infiltrative features. Tumor cell nests show decapitation secretion and glandular differentiation (H&E, ×12.5). (B) Some nests show tubular and cribriform arrangement with bloody luminal secretion (H&E, ×40). (C) Tumor cells have abundant eosinophilic cytoplasm, round to oval nuclei, dispersed chromatin and inconspicuous nuclei with frequent mitoses (H&E, ×400). (D) Deep portion of mass shows infiltrated tumor glands surround by sclerotic stroma (H&E, ×100). (E) Tumor cells are positive for CK19, suggesting origin of skin appendage (CK19, ×100). (F) High proliferation index is noted, estimating over 50% (Ki-67, ×100).
Reference
-
1. Robson A, Lazar AJ, Ben Nagi J, Hanby A, Grayson W, Feinmesser M, et al. Primary cutaneous apocrine carcinoma: a clinico-pathologic analysis of 24 cases. Am J Surg Pathol. 2008; 32:682–690.2. Costa SR, Henriques AC, Horta SH. Apocrine gland carcinoma on the right thigh. Einstein (Sao Paulo). 2008; 6:478–480.3. Katagiri Y, Ansai S. Two cases of cutaneous apocrine ductal carcinoma of the axilla. Case report and review of the literature. Dermatology. 1999; 199:332–337.4. el-Domeiri AA, Brasfield RD, Huvos AG, Strong EW. Sweat gland carcinoma: a clinico-pathologic study of 83 patients. Ann Surg. 1971; 173:270–274.5. Rutten A, Kutzner H, Mentzel T, Hantschke M, Eckert F, Angulo J, et al. Primary cutaneous cribriform apocrine carcinoma: a clinicopathologic and immunohistochemical study of 26 cases of an under-recognized cutaneous adnexal neoplasm. J Am Acad Dermatol. 2009; 61:644–651.6. Hur H, Ahn YJ, Park SH, Kim JH, Koo JS, Park BW. Clinicopathologic characteristics of apocrine breast carcinoma. J Korean Surg Soc. 2009; 77:43–49.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Nevus Sebaceus associated with Tubular Apocrine Adenoma and Apocrine Poroma
- Primary Cutaneous Mucinous Carcinoma with Extramammary Paget’s Disease: Eccrine or Apocrine?
- A Review of Studies and Experimental Methodologies on Moxibustion in Korea for an Establishment of Application Standard
- Apocrine Gland Carcinoma
- Apocrine Carcinoma of the Breast: The report of 2 cases
