The Cervical Range of Motion as a Factor Affecting Outcome in Patients With Congenital Muscular Torticollis
- Affiliations
-
- 1Department of Rehabilitation Medicine, Konkuk University School of Medicine and Konkuk University Medical Center, Seoul, Korea. kohse@kuh.ac.kr
- KMID: 2165769
- DOI: http://doi.org/10.5535/arm.2013.37.2.183
Abstract
OBJECTIVE
To investigate the factors affecting rehabilitation outcomes in children with congenital muscular torticollis (CMT).
METHODS
We retrospectively reviewed the medical records of 347 patients who were clinically suspected as having CMT and performed neck ultrasonography to measure sternocleidomastoid (SCM) muscle thickness. Fifty-four patients met the inclusion criteria. Included were demographic characteristics as well as measurements of cervical range of motion (ROM), SCM muscle thickness, and the abnormal/normal (A/N) ratio, defined as the ratio of SCM muscle thickness on the affected to the unaffected side.
RESULTS
Subjects were divided into three groups depending on degree of cervical ROM (group 1A: ROM>60, n=12; group 1B: 60> or =ROM>30, n=31; group 1C: ROM< or =30, n=11), the SCM muscle thickness (Th) (group 2A: Th<1.2 cm, n=23; group 2B: 1.2< or =Th<1.4 cm, n=18; group 2C: Th> or =1.4 cm, n=13), and the A/N ratio (R) (group 3A: R<2.2, n=19; group 3B: 2.2< or =R<2.8, n=20; group 3C: R> or =2.8, n=15). We found that more limited cervical ROM corresponded to longer treatment duration. The average treatment duration was 4.55 months in group 1A, 5.87 months in group 1B, and 6.50 months in group 1C. SCM muscle thickness and the A/N ratio were not correlated with treatment duration.
CONCLUSION
Infants with CMT who were diagnosed earlier and had an earlier intervention had a shorter duration of rehabilitation. Initial cervical ROM is an important prognostic factor for predicting the rehabilitation outcome of patients with CMT.
MeSH Terms
Figure
-
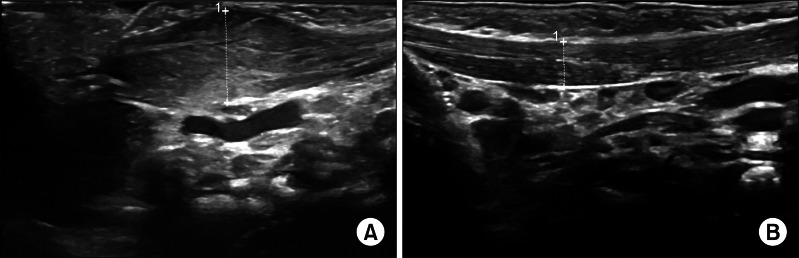
Fig. 1 Ultrasonographic features of sternocleidomastoid muscle with longitudinal view in a child with congenital muscular torticollis. (A) Sternocleidomastoid muscle of affected side shows heterogenic echotexture and fusiform dilatation. (B) Sternocleidomastoid muscle of unaffected side shows homogenous echotexture.
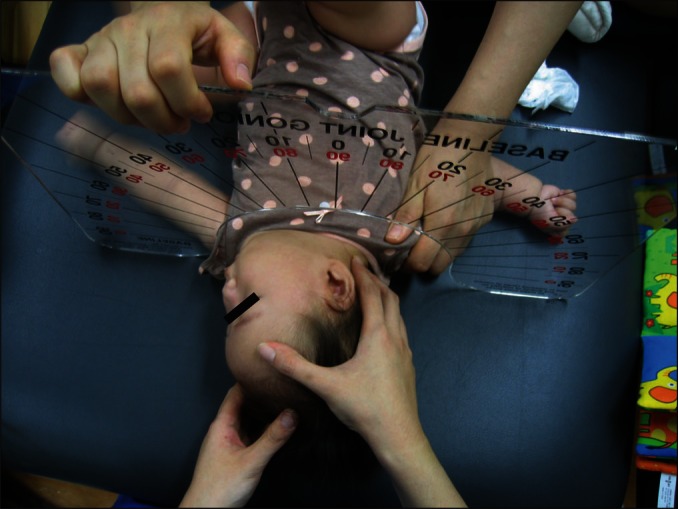
Fig. 2 Measurement of range of motion of cervical rotation.
Cited by 2 articles
-
Factors That Affect the Rehabilitation Duration in Patients With Congenital Muscular Torticollis
Ah Young Jung, Eun Young Kang, Sung Hoon Lee, Doo Hyeon Nam, Ji Hwan Cheon, Hyo Jung Kim
Ann Rehabil Med. 2015;39(1):18-24. doi: 10.5535/arm.2015.39.1.18.Clinical Usefulness of Sonoelastography in Infants With Congenital Muscular Torticollis
Seong Kyung Hong, Jin Won Song, Seung Beom Woo, Jong Min Kim, Tae Eun Kim, Zee Ihn Lee
Ann Rehabil Med. 2016;40(1):28-33. doi: 10.5535/arm.2016.40.1.28.
Reference
-
1. Cheng JC, Tang SP, Chen TM, Wong MW, Wong EM. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants: a study of 1,086 cases. J Pediatr Surg. 2000; 35:1091–1096. PMID: 10917303.2. Joyce MB, de Chalain TM. Treatment of recalcitrant idiopathic muscular torticollis in infants with botulinum toxin type A. J Craniofac Surg. 2005; 16:321–327. PMID: 15750434.
Article3. Macdonald D. Sternomastoid tumour and muscular torticollis. J Bone Joint Surg Br. 1969; 51:432–443. PMID: 5387538.
Article4. Porter SB, Blount BW. Pseudotumor of infancy and congenital muscular torticollis. Am Fam Physician. 1995; 52:1731–1736. PMID: 7484683.5. Cheng JC, Wong MW, Tang SP, Chen TM, Shum SL, Wong EM. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants: a prospective study of eight hundred and twenty-one cases. J Bone Joint Surg Am. 2001; 83-A:679–687. PMID: 11379737.6. Lee YT, Yoon K, Kim YB, Chung PW, Hwang JH, Park YS, et al. Clinical features and outcome of physiotherapy in early presenting congenital muscular torticollis with severe fibrosis on ultrasonography: a prospective study. J Pediatr Surg. 2011; 46:1526–1531. PMID: 21843719.
Article7. Cheng JC, Tang SP, Chen TM. Sternocleidomastoid pseudotumor and congenital muscular torticollis in infants: a prospective study of 510 cases. J Pediatr. 1999; 134:712–716. PMID: 10356139.
Article8. Tatli B, Aydinli N, Caliskan M, Ozmen M, Bilir F, Acar G. Congenital muscular torticollis: evaluation and classification. Pediatr Neurol. 2006; 34:41–44. PMID: 16376277.9. Wei JL, Schwartz KM, Weaver AL, Orvidas LJ. Pseudotumor of infancy and congenital muscular torticollis: 170 cases. Laryngoscope. 2001; 111(4 Pt 1):688–695. PMID: 11359141.
Article10. Do TT. Congenital muscular torticollis: current concepts and review of treatment. Curr Opin Pediatr. 2006; 18:26–29. PMID: 16470158.11. Han SJ, Shin BM, Lee JM, Yoon TS. Factors affecting rehabilitation outcome of congenital muscular torticollis. J Korean Acad Rehabil Med. 2010; 34:643–649.12. Lim D, Kwon W, Cha SW, Yoo H, Lim S, Park JM, et al. The sonographic correlation between the sternocleidomastoid muscle thickness and the prognosis of congenital muscular torticollis. J Korean Soc Radiol. 2009; 60:133–138.
Article13. Petronic I, Brdar R, Cirovic D, Nikolic D, Lukac M, Janic D, et al. Congenital muscular torticollis in children: distribution, treatment duration and outcome. Eur J Phys Rehabil Med. 2010; 46:153–157. PMID: 20485220.14. Kim SJ, Park EM, Choi WK, Seo KS, Yoon JS, Lee EH. The correlation between outcome and ultrasonographic findings in congenital muscular torticollis. J Korean Acad Rehabil Med. 2001; 25:601–608.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Familial Congenital Muscular Torticollis: A Case Report
- Ultrasonographic Findings in Torticollis
- Two Cases of Sternomastoid Tumor
- Local Botulinum Toxin Type A Injection for the Management of Congenital Muscular Torticollis
- Unipolar Release of the Sternocleidomastoideus in Congenital Muscular Torticollis in Children
