Ann Rehabil Med.
2014 Jun;38(3):421-426. 10.5535/arm.2014.38.3.421.
Compressive Radial Neuropathy Developed Under a Fibrotic Band Associated With Rhabdomyolysis and Successfully Treated With Surgery
- Affiliations
-
- 1Department of Rehabilitation Medicine, Gangnam Severance Hospital, Yonsei University Medical College, Seoul, Korea. rmpjh@yuhs.ac
- KMID: 2165764
- DOI: http://doi.org/10.5535/arm.2014.38.3.421
Abstract
- A 34-year-old male patient visited the emergency room with complaint of right wrist drop and foot drop. The day before, he was intoxicated and fell asleep in a room containing barbeque briquettes; After waking up, he noticed that his right wrist and foot were dropped. Upon physical examination, his right wrist extensor, thumb extensor, ankle dorsiflexor, and big toe extensor showed Medical Research Council (MRC) grade 1 power. The initial laboratory tests suggested rhabdomyolysis induced by unrelieved pressure on the right side during sleep. Right foot drop was improved after conservative care and elevated muscle enzyme became normalized with hydration therapy with no resultant acute renal failure. However, the wrist drop did not show improvement and a hard mass was palpated on the follow-up physical examination. Ultrasonography and magnetic resonance imaging studies were conducted and an abnormal mass in the lateral head of the tricep was detected. Axonopathy was suggested by the electrodiagnostic examination. A surgical decompression was done and a fibrotic cord lesion compressing the radial nerve was detected. After adhesiolysis, his wrist extensor power improved to MRC grade 4. Herein, we describe a compressive radial neuropathy associated with rhabdomyolysis successfully treated with surgery and provide a brief review of the related literature.
Keyword
MeSH Terms
Figure
-
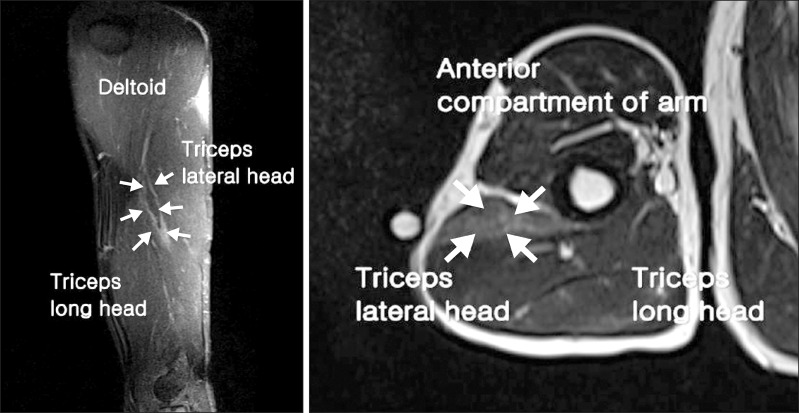
Fig. 1 Right humerus magnetic resonance imaging (2 months after onset). A high signal intensity lesion in the lateral head of the tricep muscle with peripheral enhancement pattern in the enhanced image (white arrow).
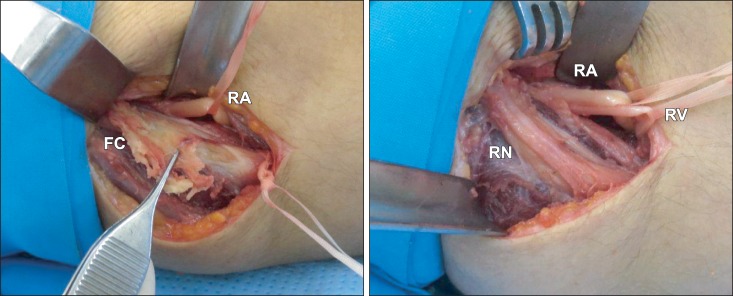
Fig. 2 Operation findings. (A) A fibrotic cord (FC) is seen. (B) After adhesiolysis, the radial nerve (RN) become visible. RA, radial artery; RV, radial vein.
Reference
-
1. Wang LH, Weiss MD. Anatomical, clinical, and electrodiagnostic features of radial neuropathies. Phys Med Rehabil Clin N Am. 2013; 24:33–47. PMID: 23177029.
Article2. Arnold WD, Krishna VR, Freimer M, Kissel JT, Elsheikh B. Prognosis of acute compressive radial neuropathy. Muscle Nerve. 2012; 45:893–895. PMID: 22581545.
Article3. Downie AW, Scott TR. An improved technique for radial nerve conduction studies. J Neurol Neurosurg Psychiatry. 1967; 30:332–336. PMID: 4293407.
Article4. Escolar DM, Jones HR Jr. Pediatric radial mononeuropathies: a clinical and electromyographic study of sixteen children with review of the literature. Muscle Nerve. 1996; 19:876–883. PMID: 8965842.
Article5. Khan FY. Rhabdomyolysis: a review of the literature. Neth J Med. 2009; 67:272–283. PMID: 19841484.6. Alterman I, Sidi A, Azamfirei L, Copotoiu S, Ezri T. Rhabdomyolysis: another complication after prolonged surgery. J Clin Anesth. 2007; 19:64–66. PMID: 17321931.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Usefulness of Proximal Radial Motor Conduction in Acute Compressive Radial Neuropathy
- Superficial Radial Neuropathy due to Anatomic Variation: A Case Report
- Rhabdomyolysis and Peripheral Neuropathy Without Compartment Syndrome, Induced by Antipsychotic Drug Intoxication: A Case Report
- Clinical Features of Wrist Drop Caused by Compressive Radial Neuropathy and Its Anatomical Considerations
- Radial Neuropathy after Cryolipolysis
