Endoscopic Management of Afferent Loop Syndrome after a Pylorus Preserving Pancreatoduodenecotomy Presenting with Obstructive Jaundice and Ascending Cholangitis
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea. bang7028@yuhs.ac
Abstract
- Afferent loop syndrome is a rare complication of gastrojejunostomy. Patients usually present with abdominal distention and bilious avomiting. Afferent loop syndrome in patients who have undergone a pylorus preserving pancreaticoduodenectomy can present with ascending cholangitis. This condition is related to a large volume of reflux through the biliary-enteric anastomosis and static materials with bacterial overgrowth in the afferent loop. Patients with afferent loop syndrome after pylorus preserving pancreaticoduodenectomy frequently cannot be confirmed as surgical candidates due to poor medical condition. In that situation, a non-surgical palliation should be considered. Herein, we report two patients with afferent loop syndrome presenting with obstructive jaundice and ascending cholangitis. The patients suffered from the recurrence of pancreatic cancer after pylorus preserving pancreaticoduodenectomy. The diagnosis of afferent loop syndrome was confirmed, and the patients were successfully treated by inserting an endoscopic metal stent using a colonoscopic endoscope.
Keyword
MeSH Terms
Figure
-

Fig. 1 Radiologic findings. (A) Abdominal X-ray shows normal bowel gas pattern. (B) Computed tomography (CT) scan shows intrahepatic duct dilatation with increased tumor size (arrow). (C) CT scan shows small bowel distention due to small bowel obstruction. (D) Cholangiogram shows intrahepatic duct dilatation and the contrast does not pass through the small bowel (arrow).

Fig. 2 Endoscopic and fluoroscopic findings. (A) Endoscopy can not pass through the lumen. (B) A metal stent (Hanaro stent, uncovered, 6 cm) is inserted through the afferent loop. (C) The dye is drained well after stent insertion. (D) A dilated afferent loop of the small bowel is noted through the restored lumen of the occluded afferent loop.
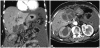
Fig. 3 Radiologic findings. (A) Computed tomography scan shows anastomotic jejunal segment dilatation. (B) It shows anastomotic jejunal segment dilatation and hydronephrosis of the right kidney.

Fig. 4 Endoscopic and fluoroscopic findings. (A) Through colonoscopic approach, cannulation is done. (B) After injection of contrast material, dye is not pass out and small bowel obstruction is noted. From biliary tract to small bowel, there is no obstruction. (C) A metal stent (Niti-S D type stent, uncovered, 10 cm) is inserted through the afferent loop. (D) The dye is drained well after stent insertion.
Reference
-
1. Woodfield CA, Levine MS. The postoperative stomach. Eur J Radiol. 2005; 53:341–352. PMID: 15741008.
Article2. Aimoto T, Uchida E, Nakamura Y, et al. Malignant afferent loop obstruction following pancreaticoduodenectomy: report of two cases. J Nihon Med Sch. 2006; 73:226–230. PMID: 16936449.
Article3. Burdick JS, Garza AA, Magee DJ, Dykes C, Jeyarajah R. Endoscopic management of afferent loop syndrome of malignant etiology. Gastrointest Endosc. 2002; 55:602–605. PMID: 11923786.
Article4. Warrier RK, Steinheber FU. Afferent loop obstruction presenting as obstructive jaundice. Dig Dis Sci. 1979; 24:74–76. PMID: 428293.
Article5. Yao NS, Wu CW, Tiu CM, Liu JM, Whang-Peng J, Chen LT. Percutaneous transhepatic duodenal drainage as an alternative approach in afferent loop obstruction with secondary obstructive jaundice in recurrent gastric cancer. Cardiovasc Intervent Radiol. 1998; 21:350–353. PMID: 9688809.
Article6. Spiliotis J, Karnabatidis D, Vaxevanidou A, et al. Acute cholangitis due to afferent loop syndrome after a Whipple procedure: a case report. Cases J. 2009; 2:6339. PMID: 19918578.
Article7. Hishinuma S, Ogata Y, Matsui J, Ozawa I. Complications after pyloruspreserving pancreatoduodenectomy with gastrointestinal reconstruction by the Imanaga method. J Am Coll Surg. 1998; 186:10–16. PMID: 9449595.
Article8. Beger HG, Treitschke F, Gansauge F, Harada N, Hiki N, Mattfeldt T. Tumor of the ampulla of Vater: experience with local or radical resection in 171 consecutively treated patients. Arch Surg. 1999; 134:526–532. PMID: 10323425.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Experience of septic shock after percutaneous management of obstructed afferent loop with obstructive jaundice: 3 cases report
- A Case of Afferent Loop Syndrome with Acute Cholangitis Developed after Percutaneous Transhepatic Cholangioscopic Lithotripsy for Treatment of Choledocholithiasis in a Patient Who Underwent Billroth II Gastrectomy
- A Case of Afferent Loop Syndrome Treated by Endoscopic Metal Stent Insertion Using Two Endoscopes
- Balloon dilation of jejunal afferent loop functional stenosis following left hepatectomy and hepaticojejunostomy long time after pylorus-preserving pancreaticoduodenectomy: a case report
- Endoscopic approaches to afferent and Roux-en-Y limb obstruction
