A Case of Afferent Loop Syndrome with Acute Cholangitis Developed after Percutaneous Transhepatic Cholangioscopic Lithotripsy for Treatment of Choledocholithiasis in a Patient Who Underwent Billroth II Gastrectomy
- Affiliations
-
- 1Department of Internal Medicine, Inha University School of Medicine, Incheon, Korea. inos@inha.ac.kr
- 2Department of Radiology, Inha University School of Medicine, Incheon, Korea.
- KMID: 1792824
- DOI: http://doi.org/10.4166/kjg.2012.59.2.180
Abstract
- Afferent loop syndrome is a rare complication which can occur in patients with Billroth II gastrectomy. Bile and pancreatic juice is congested at afferent loop in the syndrome. This syndrome can progress rapidly to necrosis, perforation, or severe sepsis, and therefore early diagnosis and swift surgical intervention is important. But, cases of endoscopic or percutaneous transhepatic drainage have been reported when surgical management was inappropriate to proceed. We report a case of afferent loop syndrome accompanying acute cholangitis developed after percutaneous transhepatic cholangioscopic lithotripsy for the retrieval of common bile duct stone in a patient who underwent Billroth II gastrectomy due to early gastric cancer. There was no other organic cause. We treated afferent loop syndrome successfully by performing balloon dilation of afferent loop outlet.
MeSH Terms
-
Acute Disease
Afferent Loop Syndrome/*etiology
Aged, 80 and over
Balloon Dilation
Cholangiography
Cholangitis/*etiology
Choledocholithiasis/*diagnosis/radiography/therapy
Common Bile Duct
Gallstones/*diagnosis/therapy
Gastroenterostomy
Humans
Lithotripsy/*adverse effects
Male
Stomach Neoplasms/surgery
Tomography, X-Ray Computed
Figure
-

Fig. 1 Percutaneous transhepatic cholangiographic finding. A single round filling defect was observed alongside mild luminal narrowing of distal common bile duct in the common bile duct.
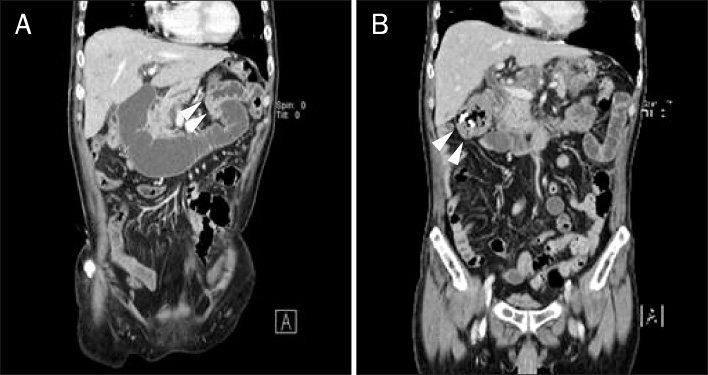
Fig. 2 Abdominal CT findings. (A) Markedly dilated afferent loop was filled with water, and the lumen of the afferent loop outlet was twisted without any luminal lesions (arrowheads). (B) Follow-up CT showed the decompressed afferent loop. Two plastic stents were migrated spontaneously and showed in the transverse colon (arrowheads).

Fig. 3 Endoscopic findings. (A) The outlet of the afferent loop was twisted (arrowheads). (B) There was no specific mucosal lesion at the afferent loop outlet dilated after balloon dilation.
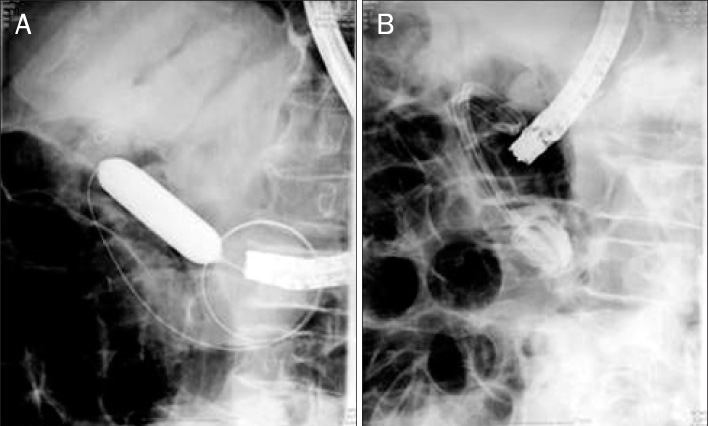
Fig. 4 Fluoroscopic findings. (A) The outlet of the afferent loop was dilated using balloon dilation catheter. (B) Two double pig-tailed plastic stents were placed in the afferent loop outlet.
Reference
-
1. Braun H. Uber Gastro-enterostomie und gleichzeitig ausgefuhrte. Entero-anastomose. Arch Klin Chir. 1893. 45:361.2. Zissin R, Hertz M, Paran H, Osadchy A, Gayer G. Computed tomographic features of afferent loop syndrome: pictorial essay. Can Assoc Radiol J. 2005. 56:72–78.3. Fisher JE, Fegelman E, Johannigman J. Schwartz SI, editor. Surgical complications. Principles of Surgery. 1999. 7th ed. New York: McGraw-Hill;441–484.4. Aoki M, Saka M, Morita S, Fukagawa T, Katai H. Afferent loop obstruction after distal gastrectomy with Roux-en-Y reconstruction. World J Surg. 2010. 34:2389–2392.5. Woodward ER. The pathophysiology of afferent loop syndrome. Surg Clin North Am. 1966. 46:411–423.6. Kim HC, Han JK, Kim KW, et al. Afferent loop obstruction after gastric cancer surgery: helical CT findings. Abdom Imaging. 2003. 28:624–630.7. Paulsen O, Skjennald A, Osnes M. An endoscopic drainage procedure for afferent loop occlusion. Gastrointest Endosc. 1987. 33:125–126.8. Park SJ, Kang HH, Park IG, et al. Two cases of afferent loop syndrome accompanying acute pancreatitis. Korean J Gastroenterol. 2001. 38:296–299.9. Burdick JS, Garza AA, Magee DJ, Dykes C, Jeyarajah R. Endoscopic management of afferent loop syndrome of malignant etiology. Gastrointest Endosc. 2002. 55:602–605.10. Kim HJ, Kim JW, Kim KH, et al. A case of afferent loop syndrome treated by endoscopic drainage procedure using nasogastric tube. Korean J Gastroenterol. 2007. 49:173–176.11. Yao NS, Wu CW, Tiu CM, Liu JM, Whang-Peng J, Chen LT. Percutaneous transhepatic duodenal drainage as an alternative approach in afferent loop obstruction with secondary obstructive jaundice in recurrent gastric cancer. Cardiovasc Intervent Radiol. 1998. 21:350–353.12. Kim YH, Han JK, Lee KH, Kim TK, Kim KW, Choi BI. Palliative percutaneous tube enterostomy in afferent-loop syndrome presenting as jaundice: clinical effectiveness. J Vasc Interv Radiol. 2002. 13:845–849.13. Carbognin G, Biasiutti C, El-Khaldi M, Ceratti S, Procacci C. Afferent loop syndrome presenting as enterolith after Billroth II subtotal gastrectomy: a case report. Abdom Imaging. 2000. 25:129–131.14. Perry T Jr. Post-gastrectomy proximal jejunal loop obstruction simulating acute pancreatitis. Ann Surg. 1954. 140:119–121.15. Bubrick MP, Hitchcock CR. Renal cyst causing afferent loop obstruction and acute pancreatitis. Am Surg. 1975. 41:440–443.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Cholangioscopic Lithotripsy for Afferent Loop Syndrome Caused by Enterolith Development after Roux-en-Y Hepaticojejunostomy: A Case Report
- Acute Abdomen Caused by Complicated Afferent Loop Syndrome after Gastrectomy
- Percutaneous transhepatic afferent loop balloon dilatation and indwelling catheter placement for benign afferent loop obstruction
- A Case of Afferent Loop Syndrome Treated by Endoscopic Drainage Procedure using Nasogastric Tube
- A Case of Afferent Loop Syndrome after Inserting a Double-Layered Pyloric Stent for Gastric Outlet Obstruction in a Patient with Stump Gastric Cancer after Undergoing Billroth II Radical Subtotal Gastrectomy
