Gastric Somatostatinoma: An Extremely Rare Cause of Upper Gastrointestinal Bleeding
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Siriraj Hospital, Mahidol University Faculty of Medicine, Bangkok, Thailand. kaiyjr@gmail.com
- 2Liver and Digestive Institute, Samitivej Sukhumvit Hospital, Bangkok, Thailand.
- 3Department of Pathology, Siriraj Hospital, Mahidol University Faculty of Medicine, Bangkok, Thailand.
Abstract
- A 49-year-old woman presented with chronic abdominal discomfort, significant weight loss, and chronic intermittent diarrhea. She suddenly developed massive upper gastrointestinal bleeding and was referred for further treatment. Endoscopy indicated a large mass in the upper gastric body with antral and duodenal bulb involvement. Endosonography showed a large well-defined isoechoic gastric subepithelial mass with multiple intra-abdominal and peripancreatic lymphadenopathy, suspected to be malignant on the basis of fine needle aspiration cytology. The tumor was surgically removed, and histopathology showed typical characteristics of a neuroendocrine tumor. On the basis of immunohistochemical staining, somatostatinoma, a rare neuroendocrine tumor, was diagnosed. Gastrointestinal bleeding is a rare presentation and the stomach is an uncommon tumor location.
MeSH Terms
Figure
-
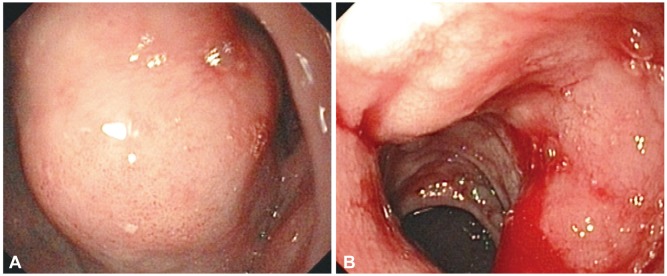
Fig. 1 Endoscopic view showing (A) a large subepithelial gastric mass and (B) duodenal invasion with bleeding.
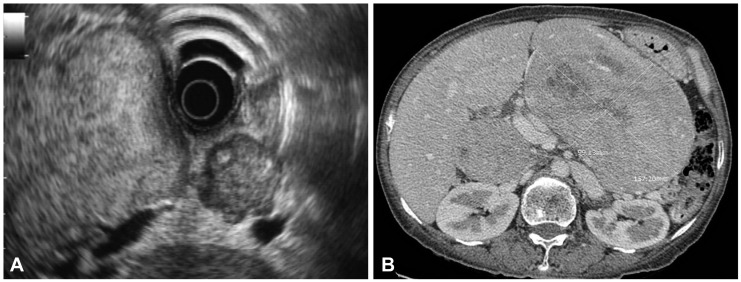
Fig. 2 (A) Endosonographic view showing a large isoechoic mass arising from the third and fourth layer, heterogeneous hypoechoic lymph nodes, suspected metastatic lymph nodes. (B) A computed tomography scan showing a large gastric mass with peripancreatic lymphadenopathy.
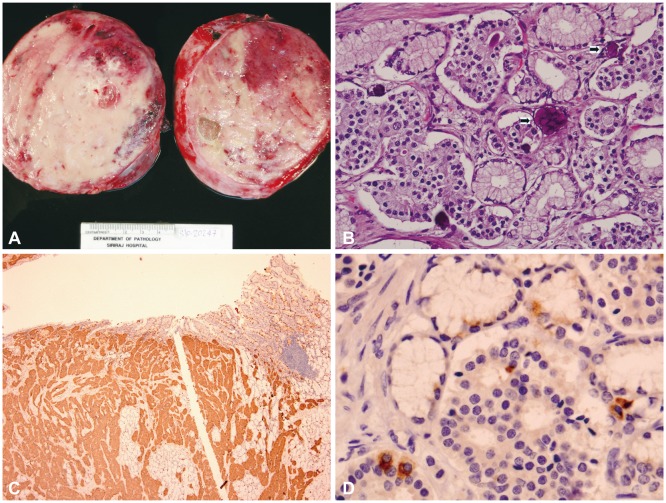
Fig. 3 (A) Gross pathology showing a tan-colored rounded mass with a rubbery consistency and whitish streaks of fibrosis. (B) Histopathology showing tumor cells with salt and pepper nuclear chromatin (H&E stain, ×20). The tumor was arranged in solid nests or in an acinar pattern. The tumor cells were cuboidal with ample granular eosinophilic cytoplasm including characteristic histologic feature of psammoma bodies (arrows) which supported somatostatinoma. (C) Synaptophysin showed diffuse positivity in the cytoplasm (×4). (D) Somatostatin staining showing a positive result (×40).
Reference
-
1. Larsson LI, Hirsch MA, Holst JJ, et al. Pancreatic somatostatinoma: clinical features and physiological implications. Lancet. 1977; 1:666–668. PMID: 66472.2. Zhang ZY, Zhang R, Wang L, et al. Diagnosis and treatment of pancreatic somatostatinoma: a case report. Chin Med J (Engl). 2008; 121:2363–2365. PMID: 19080351.
Article3. Pernet C, Kluger N, Du-Thanh A, et al. Somatostatin-producing endocrine tumour of the duodenum associated with type 1 neurofibromatosis. Acta Derm Venereol. 2010; 90:320–321. PMID: 20526564.
Article4. Arima H, Natsugoe S, Maemura K, et al. Asymptomatic somatostatinoma of the pancreatic head: report of a case. Surg Today. 2010; 40:569–573. PMID: 20496141.
Article5. Yu RS, Chen Y, Wang LH, Xu XF, Jiang DY. A large functional somatostatinoma in the pancreatic tail: atypical CT appearances. Turk J Gastroenterol. 2009; 20:291–294. PMID: 20084576.
Article6. Williamson JM, Thorn CC, Spalding D, Williamson RC. Pancreatic and peripancreatic somatostatinomas. Ann R Coll Surg Engl. 2011; 93:356–360. PMID: 21943457.
Article7. Zhang B, Xie QP, Gao SL, Fu YB, Wu YL. Pancreatic somatostatinoma with obscure inhibitory syndrome and mixed pathological pattern. J Zhejiang Univ Sci B. 2010; 11:22–26. PMID: 20043348.
Article8. Cao XP, Liu YY, Xiao HP, Li YB, Wang LT, Xiao P. Pancreatic somatostatinoma characterized by extreme hypoglycemia. Chin Med J (Engl). 2009; 122:1709–1712. PMID: 19719976.9. Colović RB, Matić SV, Micev MT, Grubor NM, Atkinson HD, Latincić SM. Two synchronous somatostatinomas of the duodenum and pancreatic head in one patient. World J Gastroenterol. 2009; 15:5859–5863. PMID: 19998510.10. Musumba CO, Usman-Saeed M, O'Toole P, Powell S, Smart HL. Persistent severe gastrointestinal bleeding in a man with metastatic somatostatinoma. Gut. 2012; 61:277–328. PMID: 21940726.
Article11. Saifuddin T, Linder C, Banerjee B. Duodenal somatostatinoma presenting as upper gastrointestinal bleeding. Am J Gastroenterol. 1999; 94:1405–1408. PMID: 10235228.
Article12. Rios A, Fernandez JA, Rodríguez JM, Lujan JA, Martínez E, Parrilla P. Massive upper gastrointestinal bleeding as a manifestation of somatostatinoma of the ampulla of vater. Dig Dis Sci. 2001; 46:2162–2165. PMID: 11680591.13. Prachayakul V, Aswakul P, Pongprasobchai S, et al. Clinical characteristics, endosonographic findings and etiologies of gastroduodenal subepithelial lesions: a Thai referral single center study. J Med Assoc Thai. 2012; 95(Suppl 2):S61–S67. PMID: 22574531.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Gastric Carcinoid Tumor with Massive Bleeding).
- Mature Cystic Gastric Teratoma in an Infant: A Case Presenting with a Gastrointestinal Bleeding
- Endoscopic Hemoclipping Treatment for Gastric Dieulafoy Lesion in a Newborn
- A Case of a Y-shaped Pedunculated Gastric Polyp Presenting as an Upper Gastrointestinal Bleeding in a Patient with Chronic Renal Failure
- Combined Upper Gastrointestinal Lesions with Esophageal Varices
