Allergy Asthma Respir Dis.
2016 May;4(3):225-229. 10.4168/aard.2016.4.3.225.
Intravenous immunoglobulin therapy in a selective IgG3 deficient patient with recurrent respiratory infections and asthma attacks
- Affiliations
-
- 1Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea. jwjung@cau.ac.kr
- KMID: 2165087
- DOI: http://doi.org/10.4168/aard.2016.4.3.225
Abstract
- The IgG subclass deficiency is defined as a significant decrease in the serum concentrations of one or more subclasses of IgG in a patient whose total IgG concentration is normal. IgG subclass deficiency can predispose to recurrent sinopulmonary infections. A 29-year-old female patient with a 4-year history of bronchial asthma presented with cough, sputum, dyspnea, and recurrent respiratory infections. She had frequently been treated with antibiotics and systemic steroids for recurrent respiratory infections and acute asthma exacerbations. Chest X-ray and computed tomography showed pectus excavatum and bronchial wall thickening without lung parenchymal abnormalities. On immunological evaluation, she was found to have a low serum IgG3, with normal total IgG concentration. Under diagnosis of selective IgG3 deficiency, she was started on monthly infusions of intravenous immunoglobulin (IVIG) therapy. The frequency and severity of respiratory infections and acute asthma exacerbations were markedly decreased during 3 years of IVIG therapy. Our case report suggests that a patient who has underlying selective IgG3 deficiency and asthma may benefit from IVIG therapy as this can significantly reduce the incidence and severity of recurrent respiratory infections and acute asthma exacerbations.
Keyword
MeSH Terms
-
Adult
Anti-Bacterial Agents
Asthma*
Cough
Diagnosis
Dyspnea
Female
Funnel Chest
Humans
IgG Deficiency
Immunization, Passive*
Immunoglobulin G*
Immunoglobulins*
Immunoglobulins, Intravenous
Incidence
Lung
Respiratory Tract Infections*
Sputum
Steroids
Thorax
Anti-Bacterial Agents
Immunoglobulin G
Immunoglobulins
Immunoglobulins, Intravenous
Steroids
Figure
-
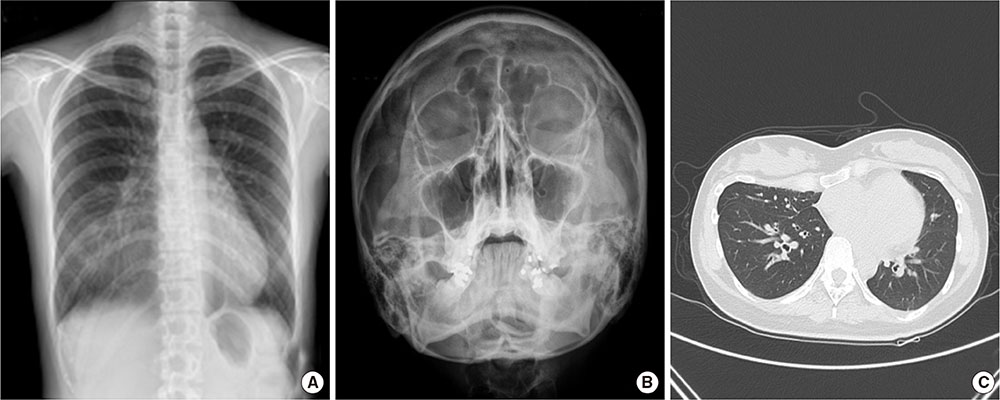
Fig. 1 (A) Chest X-ray shows increased opacity in right lower lung field, probably due to pectus excavatum. (B) Paranasal sinus waters view shows no abnormality in paranasal sinuses. (C) High resolution computed tomography of chest reveals crowding of subsegmental bronchi, medial segment of right middle lobe, probably due to pectus excavatum and bronchial wall thickening without lung parenchymal abnormalities.
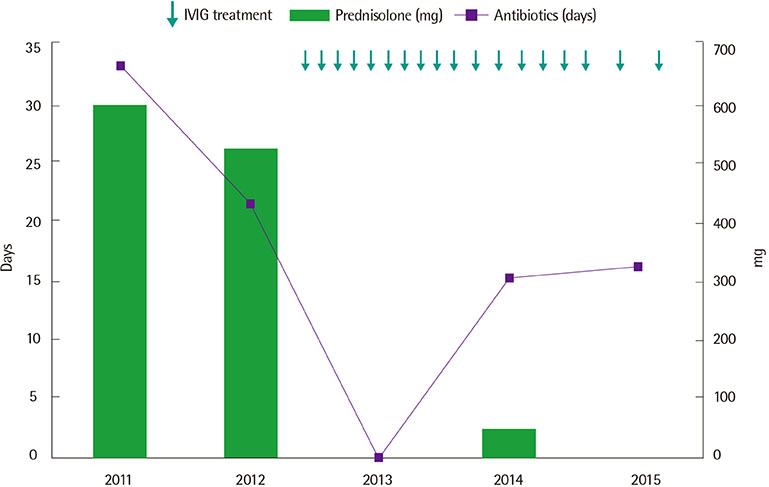
Fig. 2 Changes in duration of antibiotics and total dose of systemic steroids per year according to intravenous immunoglobulin (IVIG) treatment.
Reference
-
1. Herrod HG. Clinical significance of IgG subclasses. Curr Opin Pediatr. 1993; 5:696–699.
Article2. Hill SL, Mitchell JL, Burnett D, Stockley RA. IgG subclasses in the serum and sputum from patients with bronchiectasis. Thorax. 1998; 53:463–468.
Article3. Knutsen AP. Spectrum of antibody deficiency disorders with normal or near-normal immunoglobulin levels. Pediatr Asthma Allergy Immunol. 2006; 19:51–62.
Article4. Kim JH, Park HJ, Choi GS, Kim JE, Ye YM, Nahm DH, et al. Immunoglobulin G Subclass Deficiency is the Major Phenotype of Primary Immunodeficiency in a Korean Adult Cohort. J Korean Med Sci. 2010; 25:824–828.
Article5. Buckley RH. Immunoglobulin G subclass deficiency: fact or fancy? Curr Allergy Asthma Rep. 2002; 2:356–360.
Article6. Chong CY, Lee TL, Ho MH, Lee SL, Lau YL. Review of IgG subclass and IgA deficiency in a tertiary center. HK J Paediatr. 2006; 11:205–209.7. de Moraes Lui C, Oliveira LC, Diogo CL, Kirschfink M, Grumach AS. Immunoglobulin G subclass concentrations and infections in children and adolescents with severe asthma. Pediatr Allergy Immunol. 2002; 13:195–202.
Article8. Oxelius VA. Serum IgG and IgG subclass contents in different Gm phenotypes. Scand J Immunol. 1993; 37:149–153.
Article9. Abrahamian F, Agrawal S, Gupta S. Immunological and clinical profile of adult patients with selective immunoglobulin subclass deficiency: response to intravenous immunoglobulin therapy. Clin Exp Immunol. 2010; 159:344–350.
Article10. Bonilla FA, Khan DA, Ballas ZK, Chinen J, Frank MM, Hsu JT, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. 2015; 136:1186–1205. e1–e78.
Article11. Orange JS, Ballow M, Stiehm ER, Ballas ZK, Chinen J, De La Morena M, et al. Use and interpretation of diagnostic vaccination in primary immunodeficiency: a working group report of the Basic and Clinical Immunology Interest Section of the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2012; 130:3 Suppl. S1–24.12. Shearer WT, Buckley RH, Engler RJ, Finn AF Jr, Fleisher TA, Freeman TM, et al. Practice parameters for the diagnosis and management of immunodeficiency. The Clinical and Laboratory Immunology Committee of the American Academy of Allergy, Asthma, and Immunology (CLIC-AAAAI). Ann Allergy Asthma Immunol. 1996; 76:282–294.
Article13. Abdou NI, Greenwell CA, Mehta R, Narra M, Hester JD, Halsey JF. Efficacy of intravenous gammaglobulin for immunoglobulin G subclass and/or antibody deficiency in adults. Int Arch Allergy Immunol. 2009; 149:267–274.
Article14. Olinder-Nielsen AM, Granert C, Forsberg P, Friman V, Vietorisz A, Bjorkander J. Immunoglobulin prophylaxis in 350 adults with IgG subclass deficiency and recurrent respiratory tract infections: a long-term follow-up. Scand J Infect Dis. 2007; 39:44–50.
Article15. Krause I, Wu R, Sherer Y, Patanik M, Peter JB, Shoenfeld Y. In vitro antiviral and antibacterial activity of commercial intravenous immunoglobulin preparations--a potential role for adjuvant intravenous immunoglobulin therapy in infectious diseases. Transfus Med. 2002; 12:133–139.
Article16. Orange JS, Grossman WJ, Navickis RJ, Wilkes MM. Impact of trough IgG on pneumonia incidence in primary immunodeficiency: a meta-analysis of clinical studies. Clin Immunol. 2010; 137:21–30.
Article17. Barlan IB, Geha RS, Schneider LC. Therapy for patients with recurrent infections and low serum IgG3 levels. J Allergy Clin Immunol. 1993; 92:353–355.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of intravenous immunoglobulin therapy in severe aspirin - sensitive asthma patient combined with IgG1 and IgG3 subclass deficiency
- A case of a patient with IgG3 subclass deficiency and recurrent fungal infection of oral cavity
- Familial IgG3 subclass deficiency: A report of two cases
- Diagnosis and treatment of immunoglobulin G subclass deficiency in a school-age child with recurrent wheezing
- Serum IgG and IgG subclass in aspirin-sensitive asthma
