Comparison of Continuous Epidural Analgesia, Patient-Controlled Analgesia with Morphine, and Continuous Three-in-One Femoral Nerve Block on Postoperative Outcomes after Total Hip Arthroplasty
- Affiliations
-
- 1Department of Orthopaedic Surgery, Okayama Medical Center, Okayama, Japan. tomonori_t31@yahoo.co.jp
- 2Department of Orthopaedic Surgery, Okayama University Hospital, Okayama, Japan.
- KMID: 2164540
- DOI: http://doi.org/10.4055/cios.2015.7.2.164
Abstract
- BACKGROUND
Postoperative pain relief can be achieved with various modalities. However, there are only few reports that have analyzed postoperative analgesic techniques in total hip arthroplasty patients. The aim of this retrospective study was to compare the postoperative outcomes of three different analgesic techniques after total hip arthroplasty.
METHODS
We retrospectively reviewed the influence of three analgesic techniques on postoperative rehabilitation after total hip arthroplasty in 90 patients divided into three groups (n = 30 patients per group). Postoperative analgesia consisted of continuous epidural analgesia (Epi group), patient-controlled analgesia with morphine (PCA group), or a continuous femoral nerve block (CFNB group). We measured the following parameters relating to postoperative outcome: visual analog scale scores, the use of supplemental analgesia, side effects, length of the hospital stay, plasma D-dimer levels, and the Harris hip score.
RESULTS
Each group had low pain scores with no significant differences between the groups. The PCA group had a lower frequency of supplemental analgesia use compared to the Epi and CFNB groups. Side effects (nausea/vomiting, inappetence) and day 7 D-dimer levels were significantly lower in the CFNB group (p < 0.05). There were no significant differences between the groups in terms of the length of the hospital stay or the Harris hip score.
CONCLUSIONS
Although there were no clinically significant differences in outcomes between the three groups, the CFNB provided good pain relief which was equal to that of the other analgesics with fewer side effects and lower D-dimer levels in hospitalized patients following total hip arthroplasty.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
*Analgesia, Epidural/methods
*Analgesia, Patient-Controlled
Analgesics, Opioid/*administration & dosage
*Arthroplasty, Replacement, Hip
Female
*Femoral Nerve
Fibrin Fibrinogen Degradation Products/analysis
Humans
Length of Stay
Male
Middle Aged
Morphine/*administration & dosage
*Nerve Block/methods
Pain, Postoperative/*prevention & control
Retrospective Studies
Treatment Outcome
Analgesics, Opioid
Fibrin Fibrinogen Degradation Products
Morphine
Figure
-
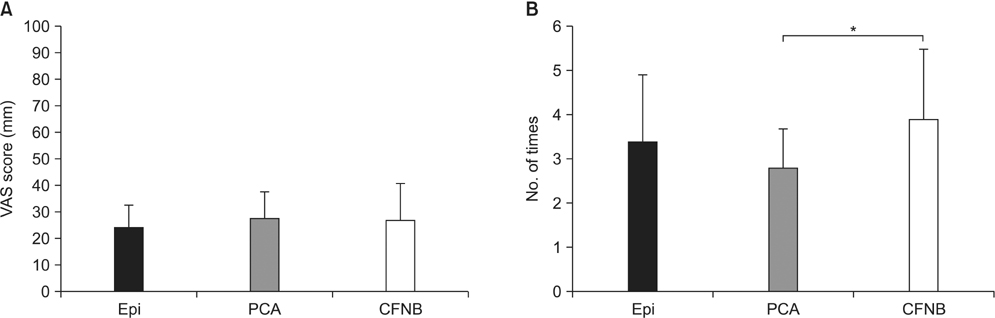
Fig. 1 (A) VAS for each group at 24 hours postoperatively. The VAS scores were not significantly different among the three groups. (B) Additional analgesic treatment was given to each of the three groups for two days after surgery. Values are presented as mean ± standard deviation. VAS: visual analog scale, Epi: epidural analgesia, PCA: patient-controlled analgesia, CFNB: continuous femoral nerve block. *p < 0.05.
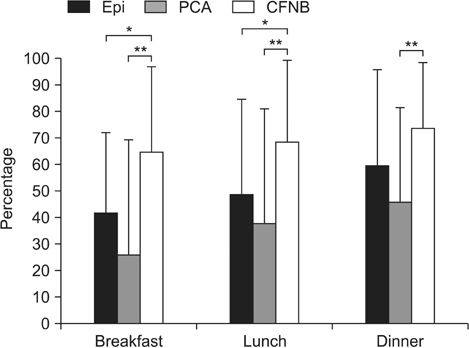
Fig. 2 Food intake of the three groups on postoperative day 1. Values are presented as mean ± standard deviation. Epi: epidural analgesia, PCA: patient-controlled analgesia, CFNB: continuous femoral nerve block. *p < 0.05. **p < 0.01.
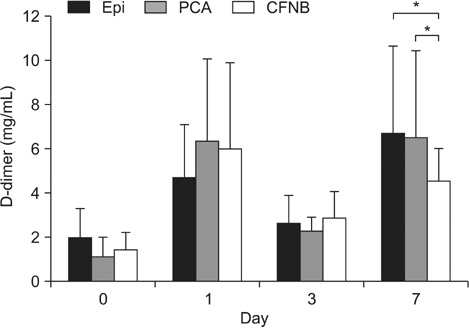
Fig. 3 D-dimer levels preoperatively (day 0) and on postoperative days 1, 3, and 7. Values are presented as mean ± standard deviation. Epi: epidural analgesia, PCA: patient-controlled analgesia, CFNB: continuous femoral nerve block. *p < 0.05.
Cited by 1 articles
-
Perioperative Pain Management in Total Hip Arthroplasty: Korean Hip Society Guidelines
Byung-Woo Min, Yeesuk Kim, Hong-Man Cho, Kyung-Soon Park, Pil Whan Yoon, Jae-Hwi Nho, Sang-Min Kim, Kyung-Jae Lee, Kyong-Ho Moon
Hip Pelvis. 2016;28(1):15-23. doi: 10.5371/hp.2016.28.1.15.
Reference
-
1. Chelly JE, Greger J, Gebhard R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty. 2001; 16(4):436–445.2. Singelyn FJ, Ferrant T, Malisse MF, Joris D. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous femoral nerve sheath block on rehabilitation after unilateral total-hip arthroplasty. Reg Anesth Pain Med. 2005; 30(5):452–457.3. Buckenmaier CC 3rd, Xenos JS, Nilsen SM. Lumbar plexus block with perineural catheter and sciatic nerve block for total hip arthroplasty. J Arthroplasty. 2002; 17(4):499–502.4. Chelly JE, Schilling D. Thromboprophylaxis and peripheral nerve blocks in patients undergoing joint arthroplasty. J Arthroplasty. 2008; 23(3):350–354.5. Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. 1998; 87(1):88–92.6. Maheshwari AV, Blum YC, Shekhar L, Ranawat AS, Ranawat CS. Multimodal pain management after total hip and knee arthroplasty at the Ranawat Orthopaedic Center. Clin Orthop Relat Res. 2009; 467(6):1418–1423.7. Sinatra RS, Torres J, Bustos AM. Pain management after major orthopaedic surgery: current strategies and new concepts. J Am Acad Orthop Surg. 2002; 10(2):117–129.8. Singelyn FJ, Gouverneur JM. Postoperative analgesia after total hip arthroplasty: i.v. PCA with morphine, patient-controlled epidural analgesia, or continuous "3-in-1" block?: a prospective evaluation by our acute pain service in more than 1,300 patients. J Clin Anesth. 1999; 11(7):550–554.9. Niimi R, Hasegawa M, Shi DQ, Sudo A. The influence of fondaparinux on the diagnosis of postoperative deep vein thrombosis by soluble fibrin and D-dimer. Thromb Res. 2012; 130(5):759–764.10. Piovella F, Wang CJ, Lu H, et al. Deep-vein thrombosis rates after major orthopedic surgery in Asia: an epidemiological study based on postoperative screening with centrally adjudicated bilateral venography. J Thromb Haemost. 2005; 3(12):2664–2670.11. Yukizawa Y, Inaba Y, Watanabe S, et al. Association between venous thromboembolism and plasma levels of both soluble fibrin and plasminogen-activator inhibitor 1 in 170 patients undergoing total hip arthroplasty. Acta Orthop. 2012; 83(1):14–21.12. Shiota N, Sato T, Nishida K, et al. Changes in LPIA D-dimer levels after total hip or knee arthroplasty relevant to deep-vein thrombosis diagnosed by bilateral ascending venography. J Orthop Sci. 2002; 7(4):444–450.13. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987; 40(5):373–383.14. Winnie AP, Ramamurthy S, Durrani Z. The inguinal paravascular technic of lumbar plexus anesthesia: the "3-in-1 block". Anesth Analg. 1973; 52(6):989–996.15. Hunt KJ, Bourne MH, Mariani EM. Single-injection femoral and sciatic nerve blocks for pain control after total knee arthroplasty. J Arthroplasty. 2009; 24(4):533–538.16. Bellamy N, Kirwan J, Boers M, et al. Recommendations for a core set of outcome measures for future phase III clinical trials in knee, hip, and hand osteoarthritis: consensus development at OMERACT III. J Rheumatol. 1997; 24(4):799–802.17. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969; 51(4):737–755.18. Grass JA. The role of epidural anesthesia and analgesia in postoperative outcome. Anesthesiol Clin North America. 2000; 18(2):407–428.19. Lippi G, Franchini M, Targher G, Favaloro EJ. Help me, Doctor! My D-dimer is raised. Ann Med. 2008; 40(8):594–605.20. Horlocker TT, Wedel DJ, Rowlingson JC, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. 2010; 35(1):64–101.21. Christie IW, McCabe S. Major complications of epidural analgesia after surgery: results of a six-year survey. Anaesthesia. 2007; 62(4):335–341.22. Kandasami M, Kinninmonth AW, Sarungi M, Baines J, Scott NB. Femoral nerve block for total knee replacement: a word of caution. Knee. 2009; 16(2):98–100.23. Ilfeld BM, Ball ST, Gearen PF, et al. Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial. Anesthesiology. 2008; 109(3):491–501.24. Ilfeld BM, Mariano ER, Madison SJ, et al. Continuous femoral versus posterior lumbar plexus nerve blocks for analgesia after hip arthroplasty: a randomized, controlled study. Anesth Analg. 2011; 113(4):897–903.25. Baker MW, Tullos HS, Bryan WJ, Oxspring H. The use of epidural morphine in patients undergoing total knee arthroplasty. J Arthroplasty. 1989; 4(2):157–161.26. Brull R, McCartney CJ, Chan VW, El-Beheiry H. Neurological complications after regional anesthesia: contemporary estimates of risk. Anesth Analg. 2007; 104(4):965–974.27. Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ. Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg Am. 2013; 95(3):193–199.28. Modig J. Regional anaesthesia and blood loss. Acta Anaesthesiol Scand Suppl. 1988; 89:44–48.29. Modig J, Malmberg P, Karlstrom G. Effect of epidural versus general anaesthesia on calf blood flow. Acta Anaesthesiol Scand. 1980; 24(4):305–309.30. Gonano C, Leitgeb U, Sitzwohl C, Ihra G, Weinstabl C, Kettner SC. Spinal versus general anesthesia for orthopedic surgery: anesthesia drug and supply costs. Anesth Analg. 2006; 102(2):524–529.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Continuous quadratus lumborum block as part of multimodal analgesia after total hip arthroplasty: a case report
- Low concentration continuous femoral nerve block improves analgesia and functional outcomes after total knee arthroplasty in spinal anesthesia
- A Case of Pre- and Postoperative Analgesia by Continuous 3-in-1 Nerve Block in Patient with Femoral Neck Fracture
- Comparison of Continuous Epidural Analgesia with Fentanyl-Bupivacaine Versus Intravenous Patient-Controlled Analgesia with Morphine for Postoperative Pain Control
- A Comparison of Patient-Controlled Epidural Analgesia and Continuous Epidural Analgesia after Total Knee Arthroplasty in Elderly Patients over 60 Years of Age
