J Korean Med Sci.
2015 Jul;30(7):895-902. 10.3346/jkms.2015.30.7.895.
Long-term Prognosis of Paroxysmal Atrial Fibrillation and Predictors for Progression to Persistnt or Chronic Atrial Fibrillation in the Korean Population
- Affiliations
-
- 1Division of Cardiology, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea.
- 2Division of Cardiology, Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yk.on@samsung.com
- KMID: 2164474
- DOI: http://doi.org/10.3346/jkms.2015.30.7.895
Abstract
- Little is known about the long-term prognosis of or predictors for the different clinical types of atrial fibrillation (AF) in Korean populations. The aim of this study was to validate a risk stratification to assess the probability of AF progression from paroxysmal AF (PAF) to persistent AF (PeAF) or permanent AF. A total of 434 patients with PAF were consecutively enrolled (mean age; 71.7 +/- 10.7 yr, 60.6% male). PeAF was defined as episodes that are sustained > 7 days and not self-terminating, while permanent AF was defined as an ongoing long-term episode. Atrial arrhythmia during follow-up was defined as atrial premature complex, atrial tachycardia, and atrial flutter. During a mean follow-up of 72.7 +/- 58.3 months, 168 patients (38.7%) with PAF progressed to PeAF or permanent AF. The mean annual AF progression was 10.7% per year. In univariate analysis, age at diagnosis, body mass index, atrial arrhythmia during follow-up, left ventricular ejection fraction, concentric left ventricular hypertrophy, left atrial diameter (LAD), and severe mitral regurgitation (MR) were significantly associated with AF progression. In multivariate analysis, age at diagnosis (P = 0.009), atrial arrhythmia during follow-up (P = 0.015), LAD (P = 0.002) and MR grade (P = 0.026) were independent risk factors for AF progression. Patients with younger age at diagnosis, atrial arrhythmia during follow-up, larger left atrial chamber size, and severe MR grade are more likely to progress to PeAF or permanent AF, suggesting more intensive medical therapy with close clinical follow-up would be required in those patients.
MeSH Terms
-
Aged
Atrial Fibrillation/epidemiology/mortality/*pathology
Atrial Flutter/*epidemiology/mortality/pathology
Atrial Premature Complexes/*epidemiology/mortality/pathology
Disease Progression
Echocardiography
Female
Heart Atria/pathology/ultrasonography
Humans
Male
Middle Aged
Republic of Korea/epidemiology
Retrospective Studies
Tachycardia, Ectopic Atrial/*epidemiology/mortality/pathology
Tachycardia, Paroxysmal/*epidemiology/mortality/pathology
Thromboembolism/epidemiology/mortality
Treatment Outcome
Figure
-
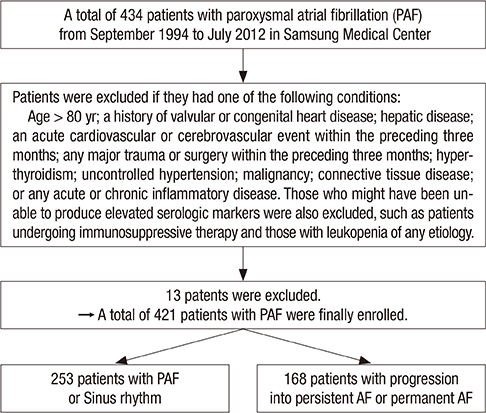
Fig. 1 Patient selection procedure.
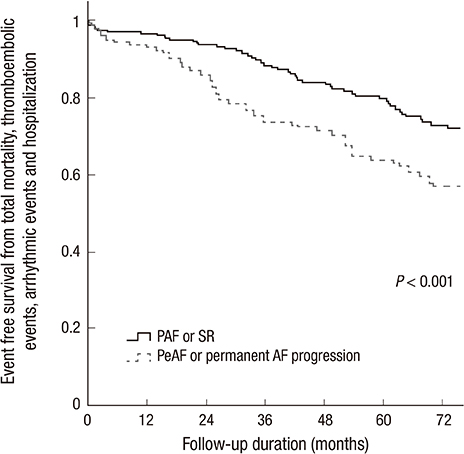
Fig. 2 Kaplan-Meier analysis for event free survival from total mortality, thromboembolic events, arrhythmic events and hospitalizations in both study groups.
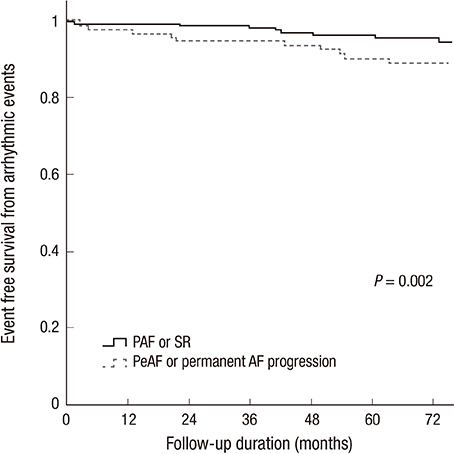
Fig. 3 Kaplan-Meier analysis for event free survival from arrhythmic events in both study groups.

Fig. 4 Progression rates from PAF to PeAF or permanent AF. *Mean annual progression rate for 6 yr-10.7%/yr.
Cited by 1 articles
-
Causal Association Between Alcohol Consumption and Atrial Fibrillation: A Mendelian Randomization Study
Jung-Ho Yang, Ji-An Jeong, Sun-Seog Kweon, Young-Hoon Lee, Seong-Woo Choi, So-Yeon Ryu, Hae-Sung Nam, Kyeong-Soo Park, Hye-Yeon Kim, Min-Ho Shin
Korean Circ J. 2022;52(3):220-230. doi: 10.4070/kcj.2021.0269.
Reference
-
1. Jahangir A, Murarka S. Progression of paroxysmal to persistent atrial fibrillation factors promoting the HATCH score. J Am Coll Cardiol. 2010; 55:732–734.2. Senoo K, Suzuki S, Otsuka T, Sagara K, Matsuno S, Kano H, Uejima T, Oikawa Y, Yajima J, Nagashima K, et al. Progression to the persistent form in asymptomatic paroxysmal atrial fibrillation. Circ J. 2014; 78:1121–1126.3. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014; 64:e1–76.4. de Vos CB, Pisters R, Nieuwlaat R, Prins MH, Tieleman RG, Coelen RJ, van den Heijkant AC, Allessie MA, Crijns HJ. Progression from paroxysmal to persistent atrial fibrillation clinical correlates and prognosis. J Am Coll Cardiol. 2010; 55:725–731.5. Kato T, Yamashita T, Sagara K, Iinuma H, Fu LT. Progressive nature of paroxysmal atrial fibrillation. Observations from a 14-year follow-up study. Circ J. 2004; 68:568–572.6. Fujiki A. Progression of atrial fibrillation from paroxysmal to persistent. Circ J. 2014; 78:1058–1060.7. Wyse DG, Gersh BJ. Atrial fibrillation: a perspective: thinking inside and outside the box. Circulation. 2004; 109:3089–3095.8. Chiang CE, Naditch-Brûlé L, Murin J, Goethals M, Inoue H, O'Neill J, Silva-Cardoso J, Zharinov O, Gamra H, Alam S, et al. Distribution and risk profile of paroxysmal, persistent, and permanent atrial fibrillation in routine clinical practice: insight from the real-life global survey evaluating patients with atrial fibrillation international registry. Circ Arrhythm Electrophysiol. 2012; 5:632–639.9. Kerr CR, Humphries KH, Talajic M, Klein GJ, Connolly SJ, Green M, Boone J, Sheldon R, Dorian P, Newman D. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2005; 149:489–496.10. Nieuwlaat R, Prins MH, Le Heuzey JY, Vardas PE, Aliot E, Santini M, Cobbe SM, Widdershoven JW, Baur LH, Lévy S, et al. Prognosis, disease progression, and treatment of atrial fibrillation patients during 1 year: follow-up of the Euro Heart Survey on atrial fibrillation. Eur Heart J. 2008; 29:1181–1189.11. Potpara TS, Stankovic GR, Beleslin BD, Polovina MM, Marinkovic JM, Ostojic MC, Lip GY. A 12-year follow-up study of patients with newly diagnosed lone atrial fibrillation: implications of arrhythmia progression on prognosis: the Belgrade Atrial Fibrillation study. Chest. 2012; 141:339–347.12. Pappone C, Radinovic A, Manguso F, Vicedomini G, Ciconte G, Sacchi S, Mazzone P, Paglino G, Gulletta S, Sala S, et al. Atrial fibrillation progression and management: a 5-year prospective follow-up study. Heart Rhythm. 2008; 5:1501–1507.13. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001; 285:2864–2870.14. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010; 137:263–272.15. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, et al. Nomenclature and Standards Committee. Task Force on Chamber Quantification. American College of Cardiology Echocardiography Committee. American Heart Association. European Association of Echocardiography, European Society of Cardiology. Recommendations for chamber quantification. Eur J Echocardiogr. 2006; 7:79–108.16. Andalib A, Brugada R, Nattel S. Atrial fibrillation: evidence for genetically determined disease. Curr Opin Cardiol. 2008; 23:176–183.17. Kubota T, Kawasaki M, Takasugi N, Imai H, Ishihara Y, Okubo M, Takahashi S, Sato H, Nishigaki K, Takemura G, et al. Left atrial pathological degeneration assessed by integrated backscatter transesophageal echocardiography as a predictor of progression to persistent atrial fibrillation: results from a prospective study of three-years follow-up. Cardiovasc Ultrasound. 2012; 10:28.18. Lu Z, Scherlag BJ, Lin J, Niu G, Fung KM, Zhao L, Ghias M, Jackman WM, Lazzara R, Jiang H, et al. Atrial fibrillation begets atrial fibrillation: autonomic mechanism for atrial electrical remodeling induced by short-term rapid atrial pacing. Circ Arrhythm Electrophysiol. 2008; 1:184–192.19. Rostock T, Steven D, Lutomsky B, Servatius H, Drewitz I, Klemm H, Müllerleile K, Ventura R, Meinertz T, Willems S. Atrial fibrillation begets atrial fibrillation in the pulmonary veins on the impact of atrial fibrillation on the electrophysiological properties of the pulmonary veins in humans. J Am Coll Cardiol. 2008; 51:2153–2160.20. Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995; 92:1954–1968.21. Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA. 1994; 271:840–844.22. DE Sisti A, Leclercq JF, Halimi F, Fiorello P, Bertrand C, Attuel P. Evaluation of time course and predicting factors of progression of paroxysmal or persistent atrial fibrillation to permanent atrial fibrillation. Pacing Clin Electrophysiol. 2014; 37:345–355.23. Gomes JA, Kang PS, Matheson M, Gough WB Jr, El-Sherif N. Coexistence of sick sinus rhythm and atrial flutter-fibrillation. Circulation. 1981; 63:80–86.24. van den Berg MP, van Gelder IC. Atrial fibrillation and sinus node dysfunction. J Am Coll Cardiol. 2001; 38:1585–1586.25. Homoud MK, Estes M 3rd. Shedding new light on the pathophysiology of conversion of paroxysmal atrial fibrillation into persistent atrial fibrillation. Am Heart J. 2007; 154:801–804.26. Huxley RR, Misialek JR, Agarwal SK, Loehr LR, Soliman EZ, Chen LY, Alonso A. Physical activity, obesity, weight change, and risk of atrial fibrillation: the Atherosclerosis Risk in Communities study. Circ Arrhythm Electrophysiol. 2014; 7:620–625.27. Hung CL, Chao TF, Lai YH, Yen CH, Wang KL, Tsao HM, Lin YJ, Chang SL, Lo LW, Hu YF, et al. The relationship among atrium electromechanical interval, insulin resistance, and metabolic syndrome. Can J Cardiol. 2013; 29:1263–1268.28. Gianfranchi L, Brignole M, Menozzi C, Lolli G, Bottoni N. Determinants of development of permanent atrial fibrillation and its treatment. Europace. 1999; 1:35–39.29. Barrett TW, Self WH, Wasserman BS, McNaughton CD, Darbar D. Evaluating the HATCH score for predicting progression to sustained atrial fibrillation in ED patients with new atrial fibrillation. Am J Emerg Med. 2013; 31:792–797.30. Schmidt EU, Schneider R, Lauschke J, Wendig I, Bänsch D. The HATCH and CHA2DS 2-VASc scores. Prognostic value in pulmonary vein isolation. Herz. 2014; 39:343–348.31. Skanes AC, Krahn AD, Yee R, Klein GJ, Connolly SJ, Kerr CR, Gent M, Thorpe KE, Roberts RS. Canadian Trial of Physiologic Pacing. Progression to chronic atrial fibrillation after pacing: the Canadian Trial of Physiologic Pacing. CTOPP Investigators. J Am Coll Cardiol. 2001; 38:167–172.32. Humphries KH, Kerr CR, Connolly SJ, Klein G, Boone JA, Green M, Sheldon R, Talajic M, Dorian P, Newman D. New-onset atrial fibrillation: sex differences in presentation, treatment, and outcome. Circulation. 2001; 103:2365–2370.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A clinical observation on antiarrhythmic efficacy of propafenone for atrial fibrillation
- Clinical significance of serum TSH in euthyroid patients with paroxysmal atrial fibrillation
- A Case of Paroxysmal Atrial Fibrillation and Sinus Bradycardia due to Coronary Artery Spasm
- The Joint Multicenter Study on the Atrial Fibrillation in Korea
- Pathophysiology and Diagnosis in Atrial Fibrillation
