Atypical Unilateral Posterior Reversible Encephalopathy Syndrome Mimicking a Middle Cerebral Artery Infarction
- Affiliations
-
- 1Department of Radiology, Ondokuz Mayis University, Faculty of Medicine, Kurupelit 55220, Samsun, Turkey. ilkayozaydin@hotmail.com
- 2Department of Neurology, Yonsei University Severance Hospital, Seoul 03722, Korea.
- 3Department of Radiology, Yonsei University Severance Hospital, Seoul 03722, Korea.
- KMID: 2160778
- DOI: http://doi.org/10.3348/kjr.2015.16.5.1104
Abstract
- Posterior reversible encephalopathy syndrome (PRES) is usually a reversible clinical and radiological entity associated with typical features on brain MR or CT imaging. However, the not-so-uncommon atypical radiological presentations of the condition are also present and they may go unrecognised as they are confused with other conditions. Here, we report a very rare case of atypical, unilateral PRES in a 49-year-old uremic, post-transplant female patient who presented with seizures. Initial MRI showed high-grade occlusion of the left middle cerebral artery (MCA) and lesions suggestive of subacute infarction in the ipsilateral frontotemporoparietal lobe. Patient symptoms had resolved a day after the onset without any specific treatment but early follow-up CT findings suggested hemorrhagic transformation. Follow-up MRI performed 2 years later showed complete disappearence of the lesions and persisting MCA occlusion.
MeSH Terms
Figure
-
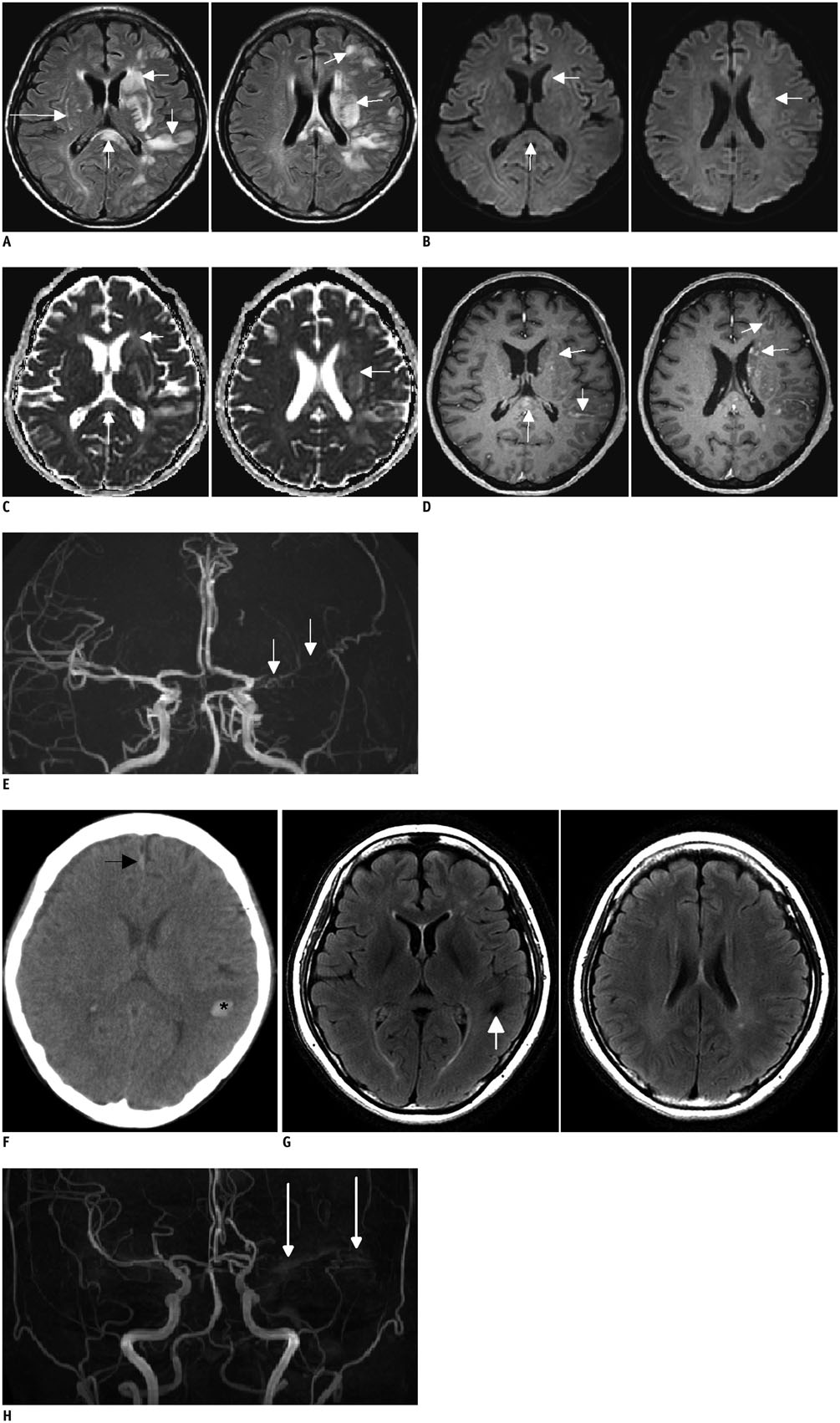
Fig. 1 Unilateral posterior reversible encephalopathy syndrome in 49-year-old woman with acute renal failure who had history of lung transplantation and of taking tacrolimus. A. Axial fluid attenuation inversion recovery images show extensive hyperintense lesions mainly in left frontotemporoparietal region predominantly involving subcortical and deep white matter including splenium of corpus callosum, and striatum (short arrows). Subtle hyperintensity is also noted in right external capsule (long arrow). B. Diffusion weighted images show that lesions are iso to hyperintense (arrows). C. Apparent diffusion coefficient maps show that lesions are hyperintense suggesting vasogenic edema (arrows). D. Post-contrast axial three-dimensional (3D)-T1 weighted images show patchy enhancement of lesions (arrows). E. 3D-time-of-flight image reveals high-grade occlusion of left middle cerebral artery (arrows). F. Follow-up CT examination of patient performed 5 days later. Axial image shows newly developed small intraparenchymal hematoma in left temporal lobe (asterisk). Right frontal subdural widening and small subarachnoid hemorrhage along right side of anterior interhemispheric fissure were also noted (arrow). Follow-up MRI performed at two years after first examination. G. Axial fluid attenuation inversion recovery images show complete disappearance of lesions and old hemorrhagic focus in left temporal lobe (arrow). H. Three-dimensional time-of-flight image shows stable left middle cerebral artery occlusion (arrows).
Reference
-
1. Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med. 1996; 334:494–500.2. Bartynski WS. Posterior reversible encephalopathy syndrome, part 1: fundamental imaging and clinical features. AJNR Am J Neuroradiol. 2008; 29:1036–1042.3. McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, et al. Posterior reversible encephalopathy syndrome: incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol. 2007; 189:904–912.4. McKinney AM, Jagadeesan BD, Truwit CL. Central-variant posterior reversible encephalopathy syndrome: brainstem or basal ganglia involvement lacking cortical or subcortical cerebral edema. AJR Am J Roentgenol. 2013; 201:631–638.5. Hugonnet E, Da Ines D, Boby H, Claise B, Petitcolin V, Lannareix V, et al. Posterior reversible encephalopathy syndrome (PRES): features on CT and MR imaging. Diagn Interv Imaging. 2013; 94:45–52.6. Schambra HM, Greer DM. Asymmetric reversible posterior leukoencephalopathy syndrome. Neurocrit Care. 2006; 4:245–247.7. Covarrubias DJ, Luetmer PH, Campeau NG. Posterior reversible encephalopathy syndrome: prognostic utility of quantitative diffusion-weighted MR images. AJNR Am J Neuroradiol. 2002; 23:1038–1048.8. Hefzy HM, Bartynski WS, Boardman JF, Lacomis D. Hemorrhage in posterior reversible encephalopathy syndrome: imaging and clinical features. AJNR Am J Neuroradiol. 2009; 30:1371–1379.9. McKinney AM, Sarikaya B, Gustafson C, Truwit CL. Detection of microhemorrhage in posterior reversible encephalopathy syndrome using susceptibility-weighted imaging. AJNR Am J Neuroradiol. 2012; 33:896–903.10. Dhar R, Dacey R, Human T, Zipfel G. Unilateral posterior reversible encephalopathy syndrome with hypertensive therapy of contralateral vasospasm: case report. Neurosurgery. 2011; 69:E1176–E1181. E118111. Voetsch B, Tarlov N, Nguyen TN, DeFusco C, Barest GD, Norbash A, et al. Asymmetric posterior reversible encephalopathy syndrome complicating hemodynamic augmentation for subarachnoid hemorrhage-associated cerebral vasospasm. Neurocrit Care. 2011; 15:542–546.12. Romano A, Silvia P, Alberto P, Tavanti F, Sette G, La Starza S, et al. Asymmetric posterior reversible encephalopathy syndrome in patient with hyperplastic anterior choroidal artery. J Headache Pain. 2011; 12:259–261.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Reversible Encephalopathy Syndrome with Extensive Brain Involvement Accompanied by Cerebral Infarction
- Reversible Cerebral Vasoconstriction Syndrome Combined with Posterior Encephalopathy Syndrome, and Transient Splenial Lesion after Delivery
- Bilateral Anterior Cerebral Artery Infarction Associated with Reversible Cerebral Vasoconstriction Syndrome
- Posterior Reversible Encephalopathy Syndrome in a Patient with Intoxication of Arisaema amurense
- Hypertensive Brainstem Encephalopathy Combined with Acute Ischemic Stroke
