Whole-Body MRI in Children: Current Imaging Techniques and Clinical Applications
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul 05505, Korea. hwgoo@amc.seoul.kr
- KMID: 2160764
- DOI: http://doi.org/10.3348/kjr.2015.16.5.973
Abstract
- Whole-body magnetic resonance imaging (MRI) is increasingly used in children to evaluate the extent and distribution of various neoplastic and non-neoplastic diseases. Not using ionizing radiation is a major advantage of pediatric whole-body MRI. Coronal and sagittal short tau inversion recovery imaging is most commonly used as the fundamental whole-body MRI protocol. Diffusion-weighted imaging and Dixon-based imaging, which has been recently incorporated into whole-body MRI, are promising pulse sequences, particularly for pediatric oncology. Other pulse sequences may be added to increase diagnostic capability of whole-body MRI. Of importance, the overall whole-body MRI examination time should be less than 30-60 minutes in children, regardless of the imaging protocol. Established and potentially useful clinical applications of pediatric whole-body MRI are described.
Keyword
MeSH Terms
Figure
-

Fig. 1 16-year-old boy with testicular rhabdomyosarcoma. A. Coronal short tau inversion recovery (STIR) whole-body magnetic resonance imaging (MRI) obtained with dual-source parallel radiofrequency excitation technology at 3T reveals residual dielectric shading artifact (arrows) at medial aspect of left buttock and thigh. B. Coronal STIR whole-body MRI obtained at 1.5T demonstrates no substantial dielectric shading artifact throughout entire body.
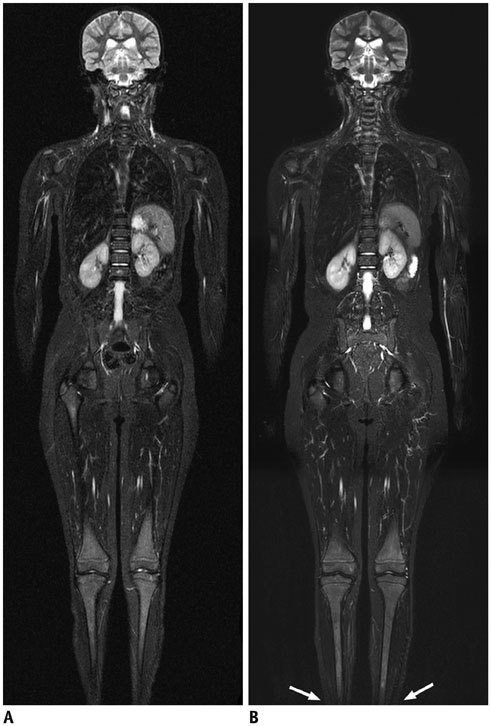
Fig. 2 11-year-old girl with Ewing sarcoma of cervical spine. Compared with coronal short tau inversion recovery (STIR) whole-body MRI obtained with quadrature body coil approach at 1.5T (A), coronal STIR whole-body MRI obtained with sliding surface coil approach at 1.5T shows higher signal-to-noise ratio and spatial resolution (B). Longitudinal coverage of sliding surface coil approach is limited by 125 cm. Thus, both legs below low calves (arrows) were not included in this case due to this limitation (B).
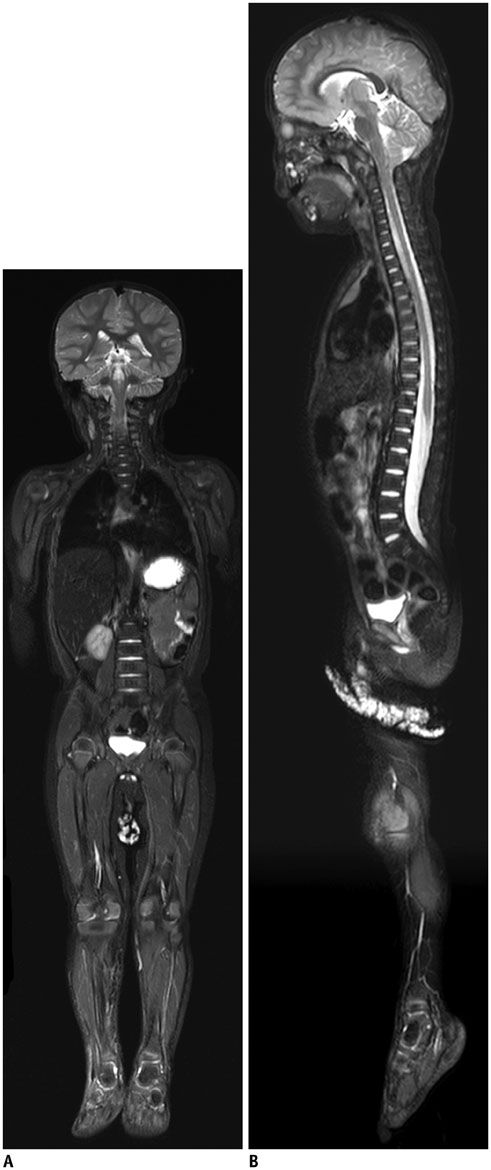
Fig. 3 2-year-old boy with infantile fibrosarcoma at craniocervical junction. Coronal (A) and sagittal (B) short tau inversion recovery whole-body magnetic resonance imaging obtained with combined neurovascular and spine coils at 3T show high signal-to-noise ratio and spatial resolution (B). Spine coils provide high signals sufficient for imaging anterior body parts of this thin, small child.

Fig. 4 Advantages of T2-weighted Dixon fast spin echo whole-body magnetic resonance imaging (MRI) in adult volunteer. Compared with coronal short tau inversion recovery whole-body MRI obtained at 3T showing incomplete fat suppression (A), coronal T2-weighted fast spin echo whole-body MRI with Dixon-based fat saturation at 3T (B) clearly demonstrates improved fat suppression throughout entire body except for left leg in lowest station (arrows) caused by fat-water swapping error. Motion artifacts in thorax and upper abdomen are less pronounced on T2-weighted fast spin echo imaging (B).

Fig. 5 1-year-old boy with neuroblastoma. Coronal T1-weighted Dixon-based fat-only (A) and water-only (B) whole-body magnetic resonance imaging at 3T shows that these two image types are swapped at second station covering thoracic region.
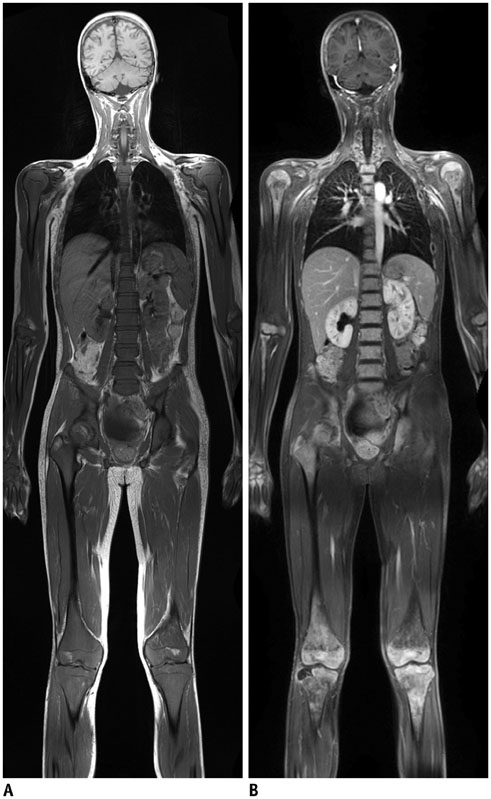
Fig. 6 14-year-old boy with leukemia. A. Coronal pre-contrast T1-weighted whole-body magnetic resonance imaging (MRI) at 1.5T shows that majority of normal fatty marrow is replaced by leukemic cells. B. Coronal post-contrast fat-saturated T1-weighted MRI at 1.5T reveals not only diffuse abnormal bone marrow enhancement but also extensive osteonecrosis in proximal humeri, distal femurs, and proximal tibias.
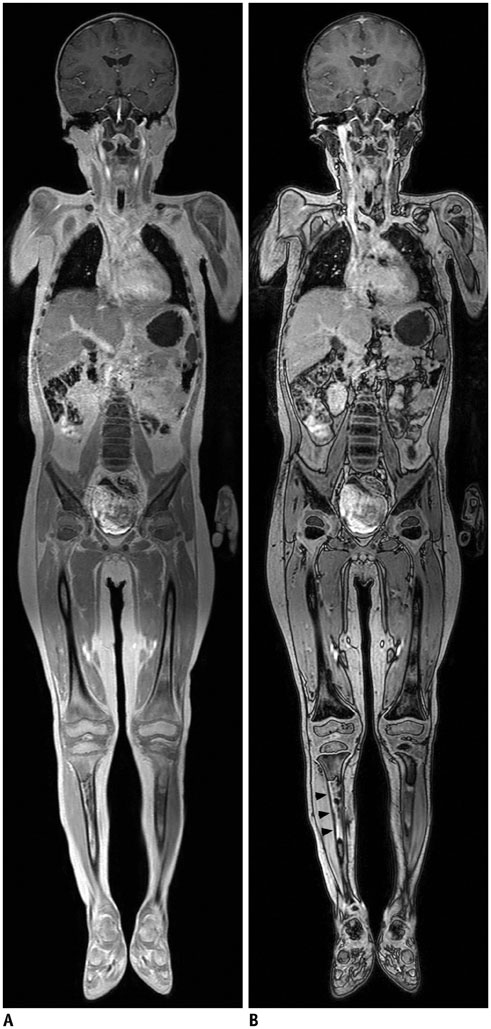
Fig. 7 4-year-old boy with B-cell lymphoma. Compared with coronal post-contrast in-phase whole-body magnetic resonance imaging (MRI) at 3T (A), normal bone marrow demonstrates dark signal intensity on coronal post-contrast opposed-phase whole-body MRI at 3T (B). In contrast, marrow-replacing lymphoma lesion in right tibia (arrowheads) remains hyperintense on opposed-phase image (B).
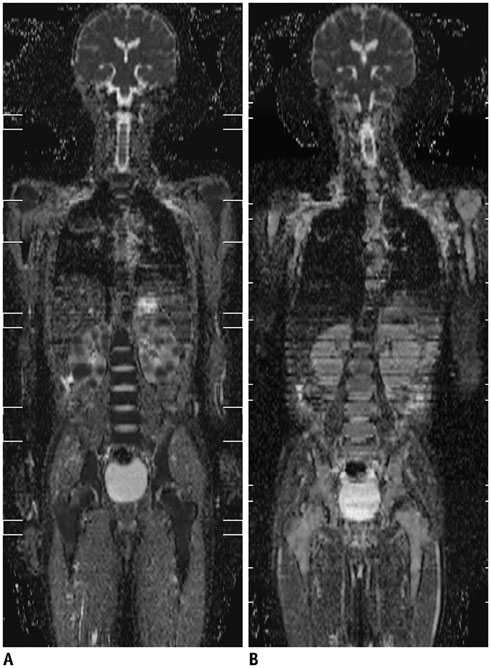
Fig. 8 10-year-old boy with Burkitt lymphoma. A. Initial coronal whole-body apparent diffusion coefficient (ADC) map at 1.5T shows restricted water diffusion in all bone marrow and multiple variable-sized renal masses, indicating viable tumors. B. Follow-up coronal whole-body ADC map at 1.5T obtained 9 days after induction chemotherapy demonstrates markedly increased water diffusion in lesions suggesting favorable treatment response.
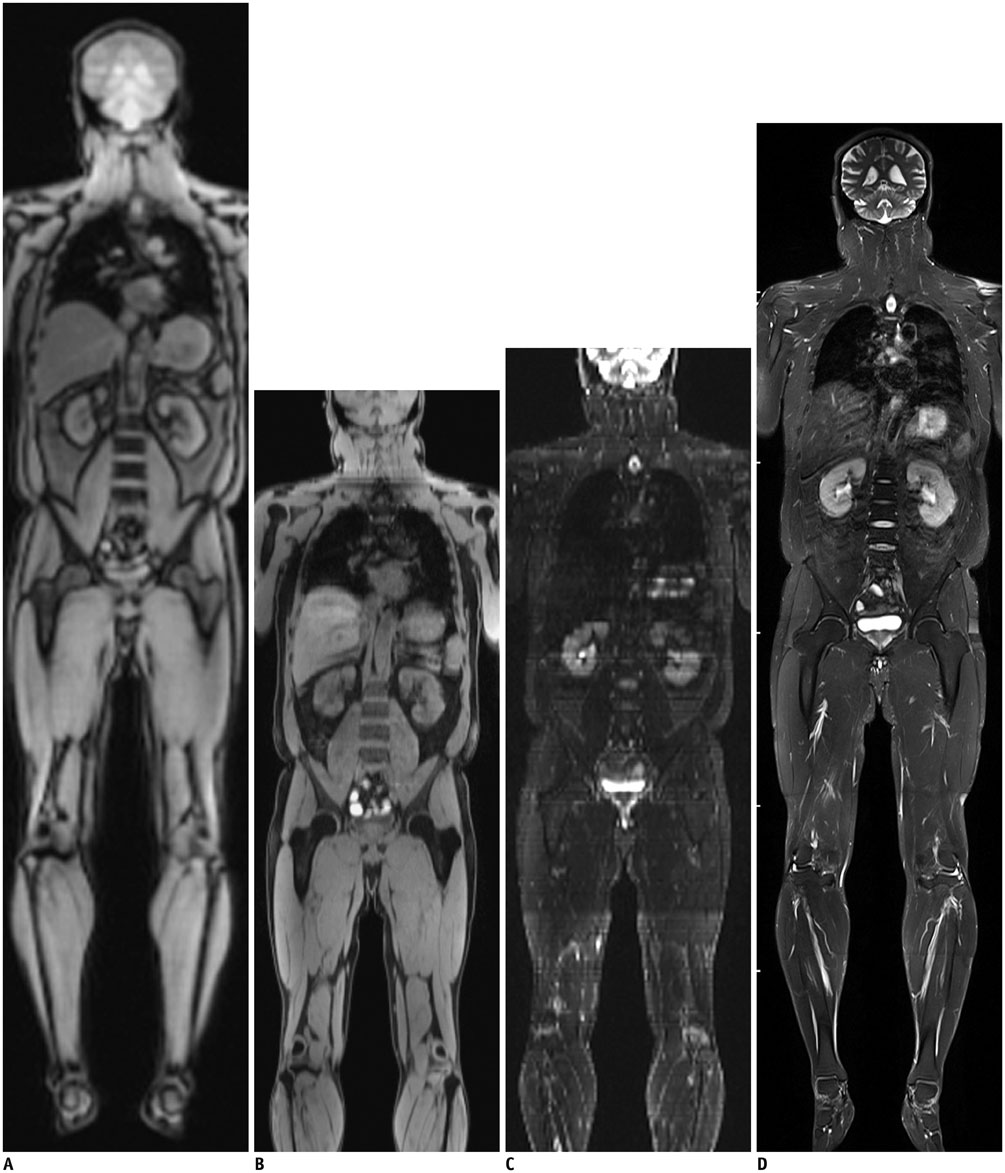
Fig. 9 Whole-body magnetic resonance imaging (MRI) using continuously moving table approach in adult volunteer. A. Low-resolution coronal reformatted fast gradient-echo whole-body MRI using continuously moving table approach (table feed, 46.9 mm/sec) at 3T was used as scout view for whole-body MRI or MR/positron emission tomography. High-resolution coronal reformatted fat-saturated T1-weighted gradient echo (B) and T2-weighted half-Fourier-acquired singe-shot turbo spin echo (C) whole-body MRIs using continuously moving table approach at 3T were obtained at much slower table feed (8.9 mm/sec). Compared with coronal Dixon-based fat-saturated T2-weighted fast spin echo whole-body MRI acquired with conventional multi-station approach (D), longitudinal coverage of high-resolution whole-body MRI acquired with continuously moving table approach is slightly limited (B, C) and stepping artifacts may degrade image quality (C).

Fig. 10 15-year-old boy with neurofibromatosis type II and plexiform schwannomas. A. Coronal short tau inversion recovery whole-body magnetic resonance imaging at 3T shows widespread plexiform schwannomas along nerve roots. Largest lesion (arrows) is noted in right suprarenal region. B. Plexiform schwannomas along cervical nerve roots are nicely delineated on curved planar reformatted post-contrast three-dimensional fluid attenuation inversion recovery image at 3T.
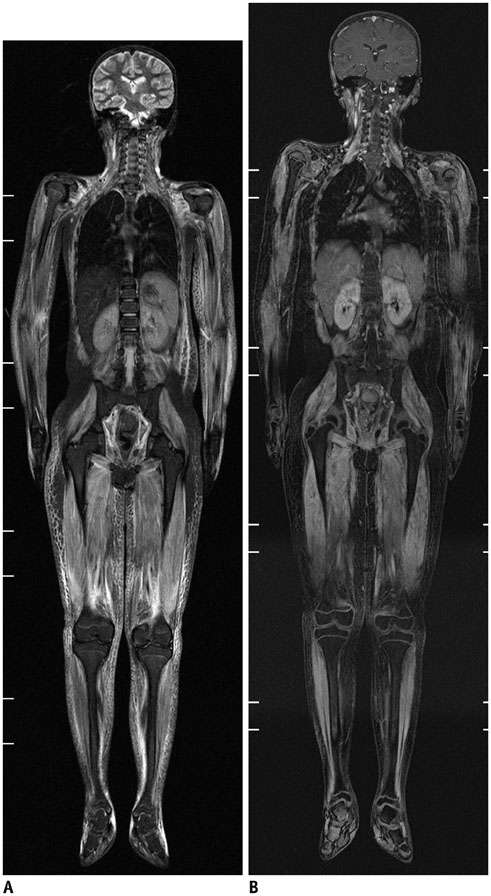
Fig. 11 10-year-old girl with juvenile dermatomyositis. A. Coronal short tau inversion recovery whole-body magnetic resonance imaging (MRI) at 1.5T reveals extensive muscular hyperintensity and reticular subcutaneous hyperintensity. B. Mild contrast enhancement in active dermatomyositis lesions is shown on coronal post-contrast fat-saturated T1-weighted gradient echo whole-body MRI at 1.5T.
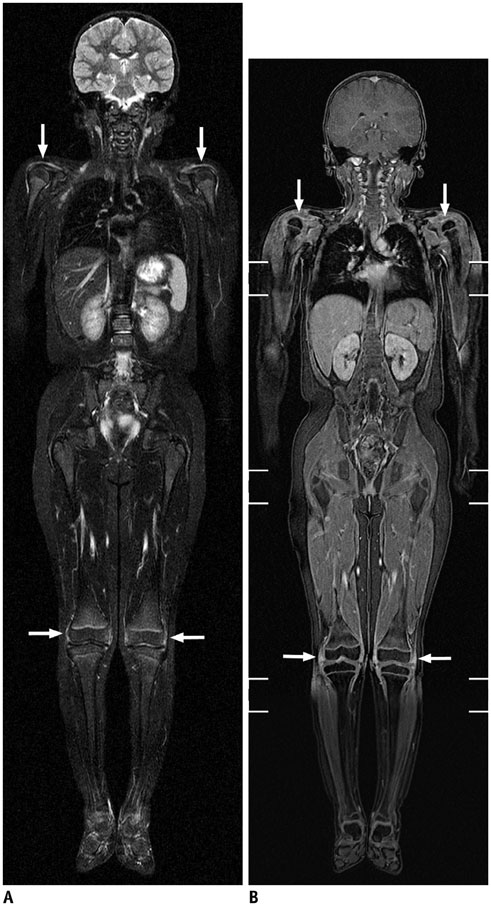
Fig. 12 6-year-old girl with juvenile rheumatoid arthritis. Coronal short tau inversion recovery (STIR) post-contrast fat-saturated coronal three-dimensional T1-weighted gradient-echo magnetic resonance image (MRI) at 1.5T. Periarticular soft tissue T2 hyperintensity and enhancement around both shoulder and knee joints (arrows) suggesting active synovitis are identified on STIR (A) and post-contrast fat-saturated T1-weighted gradient echo (B) whole-body MRIs at 1.5T.
Reference
-
1. Daldrup-Link HE, Franzius C, Link TM, Laukamp D, Sciuk J, Jürgens H, et al. Whole-body MR imaging for detection of bone metastases in children and young adults: comparison with skeletal scintigraphy and FDG PET. AJR Am J Roentgenol. 2001; 177:229–236.2. Goo HW, Choi SH, Ghim T, Moon HN, Seo JJ. Whole-body MRI of paediatric malignant tumours: comparison with conventional oncological imaging methods. Pediatr Radiol. 2005; 35:766–773.3. Goo HW, Yang DH, Ra YS, Song JS, Im HJ, Seo JJ, et al. Whole-body MRI of Langerhans cell histiocytosis: comparison with radiography and bone scintigraphy. Pediatr Radiol. 2006; 36:1019–1031.4. Punwani S, Taylor SA, Bainbridge A, Prakash V, Bandula S, De Vita E, et al. Pediatric and adolescent lymphoma: comparison of whole-body STIR half-Fourier RARE MR imaging with an enhanced PET/CT reference for initial staging. Radiology. 2010; 255:182–190.5. Goo HW. Whole-body MRI of neuroblastoma. Eur J Radiol. 2010; 75:306–314.6. Chavhan GB, Babyn PS. Whole-body MR imaging in children: principles, technique, current applications, and future directions. Radiographics. 2011; 31:1757–1772.7. Goo HW. Regional and whole-body imaging in pediatric oncology. Pediatr Radiol. 2011; 41:Suppl 1. S186–S194.8. Goo HW. High field strength magnetic resonance imaging in children. J Korean Med Assoc. 2010; 53:1093–1102.9. Willinek WA, Gieseke J, Kukuk GM, Nelles M, König R, Morakkabati-Spitz N, et al. Dual-source parallel radiofrequency excitation body MR imaging compared with standard MR imaging at 3.0 T: initial clinical experience. Radiology. 2010; 256:966–975.10. Takahara T, Kwee T, Kibune S, Ochiai R, Sakamoto T, Niwa T, et al. Whole-body MRI using a sliding table and repositioning surface coil approach. Eur Radiol. 2010; 20:1366–1373.11. Brandão S, Seixas D, Ayres-Basto M, Castro S, Neto J, Martins C, et al. Comparing T1-weighted and T2-weighted three-point Dixon technique with conventional T1-weighted fat-saturation and short-tau inversion recovery (STIR) techniques for the study of the lumbar spine in a short-bore MRI machine. Clin Radiol. 2013; 68:e617–e623.12. Costelloe CM, Madewell JE, Kundra V, Harrell RK, Bassett RL Jr, Ma J. Conspicuity of bone metastases on fast Dixon-based multisequence whole-body MRI: clinical utility per sequence. Magn Reson Imaging. 2013; 31:669–675.13. Schmidt MA. Phase-uncertainty quality map for two-point Dixon fat-water separation. Phys Med Biol. 2011; 56:N195–N205.14. Pasoglou V, Michoux N, Peeters F, Larbi A, Tombal B, Selleslagh T, et al. Whole-body 3D T1-weighted MR imaging in patients with prostate cancer: feasibility and evaluation in screening for metastatic disease. Radiology. 2015; 275:155–166.15. Dreizin D, Ahlawat S, Del Grande F, Fayad LM. Gradient-echo in-phase and opposed-phase chemical shift imaging: role in evaluating bone marrow. Clin Radiol. 2014; 69:648–657.16. Kwee TC, Takahara T, Vermoolen MA, Bierings MB, Mali WP, Nievelstein RA. Whole-body diffusion-weighted imaging for staging malignant lymphoma in children. Pediatr Radiol. 2010; 40:1592–1602. quiz 1720-172117. Padhani AR, Makris A, Gall P, Collins DJ, Tunariu N, de Bono JS. Therapy monitoring of skeletal metastases with whole-body diffusion MRI. J Magn Reson Imaging. 2014; 39:1049–1078.18. Takahara T, Imai Y, Yamashita T, Yasuda S, Nasu S, Van Cauteren M. Diffusion weighted whole body imaging with background body signal suppression (DWIBS): technical improvement using free breathing, STIR and high resolution 3D display. Radiat Med. 2004; 22:275–282.19. Chen NK, Guidon A, Chang HC, Song AW. A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage. 2013; 72:41–47.20. Filli L, Wurnig MC, Luechinger R, Eberhardt C, Guggenberger R, Boss A. Whole-body intravoxel incoherent motion imaging. Eur Radiol. 2015; 01. 10. [Epub]. DOI: 10.1007/s00330-014-3577-z.21. Klenk C, Gawande R, Uslu L, Khurana A, Qiu D, Quon A, et al. Ionising radiation-free whole-body MRI versus (18) F-fluorodeoxyglucose PET/CT scans for children and young adults with cancer: a prospective, non-randomised, single-centre study. Lancet Oncol. 2014; 15:275–285.22. Sengupta S, Smith DS, Welch EB. Continuously moving table MRI with golden angle radial sampling. Magn Reson Med. 2014; 12. 02. [Epub]. DOI: 10.1002/mrm.25531.23. Naguib NN, Bohrt K, Nour-Eldin NE, Schulz B, Tawfik AM, Siebenhandel P, et al. Whole-body MR angiography: first experiences with the new TimCT technology with single contrast injection. J Magn Reson Imaging. 2014; 39:434–439.24. Hong TS, Greer ML, Grosse-Wortmann L, Yoo SJ, Babyn PS. Whole-body MR angiography: initial experience in imaging pediatric vasculopathy. Pediatr Radiol. 2011; 41:769–778.25. Siegel MJ, Acharyya S, Hoffer FA, Wyly JB, Friedmann AM, Snyder BS, et al. Whole-body MR imaging for staging of malignant tumors in pediatric patients: results of the American College of Radiology Imaging Network 6660 Trial. Radiology. 2013; 266:599–609.26. Hirsch FW, Sattler B, Sorge I, Kurch L, Viehweger A, Ritter L, et al. PET/MR in children. Initial clinical experience in paediatric oncology using an integrated PET/MR scanner. Pediatr Radiol. 2013; 43:860–875.27. Schäfer JF, Gatidis S, Schmidt H, Gückel B, Bezrukov I, Pfannenberg CA, et al. Simultaneous whole-body PET/MR imaging in comparison to PET/CT in pediatric oncology: initial results. Radiology. 2014; 273:220–231.28. Yoo HJ, Lee JS, Lee JM. Integrated whole body MR/PET: where are we? Korean J Radiol. 2015; 16:32–49.29. Atkin KL, Ditchfield MR. The role of whole-body MRI in pediatric oncology. J Pediatr Hematol Oncol. 2014; 36:342–352.30. Lee E, Goo HW, Lee JY. Age- and gender-specific estimates of cumulative CT dose over 5 years using real radiation dose tracking data in children. Pediatr Radiol. 2015; 03. 24. [Epub]. DOI: 10.1007/s00247-015-3331-y.31. Ording Müller LS, Avenarius D, Olsen OE. High signal in bone marrow at diffusion-weighted imaging with body background suppression (DWIBS) in healthy children. Pediatr Radiol. 2011; 41:221–226.32. Kellenberger CJ, Epelman M, Miller SF, Babyn PS. Fast STIR whole-body MR imaging in children. Radiographics. 2004; 24:1317–1330.33. Littooij AS, Kwee TC, Barber I, Granata C, Vermoolen MA, Enríquez G, et al. Whole-body MRI for initial staging of paediatric lymphoma: prospective comparison to an FDG-PET/CT-based reference standard. Eur Radiol. 2014; 24:1153–1165.34. Adams HJ, Kwee TC, Lokhorst HM, Westerweel PE, Fijnheer R, Kersten MJ, et al. Potential prognostic implications of whole-body bone marrow MRI in diffuse large B-cell lymphoma patients with a negative blind bone marrow biopsy. J Magn Reson Imaging. 2014; 39:1394–1400.35. Mueller WP, Melzer HI, Schmid I, Coppenrath E, Bartenstein P, Pfluger T. The diagnostic value of 18F-FDG PET and MRI in paediatric histiocytosis. Eur J Nucl Med Mol Imaging. 2013; 40:356–363.36. Miettunen PM, Lafay-Cousin L, Guilcher GM, Nettel-Aguirre A, Moorjani V. Widespread osteonecrosis in children with leukemia revealed by whole-body MRI. Clin Orthop Relat Res. 2012; 470:3587–3595.37. Cai W, Kassarjian A, Bredella MA, Harris GJ, Yoshida H, Mautner VF, et al. Tumor burden in patients with neurofibromatosis types 1 and 2 and schwannomatosis: determination on whole-body MR images. Radiology. 2009; 250:665–673.38. Monsalve J, Kapur J, Malkin D, Babyn PS. Imaging of cancer predisposition syndromes in children. Radiographics. 2011; 31:263–280.39. Yang DH, Goo HW. Generalized lymphangiomatosis: radiologic findings in three pediatric patients. Korean J Radiol. 2006; 7:287–291.40. Malattia C, Damasio MB, Madeo A, Pistorio A, Providenti A, Pederzoli S, et al. Whole-body MRI in the assessment of disease activity in juvenile dermatomyositis. Ann Rheum Dis. 2014; 73:1083–1090.41. Quijano-Roy S, Avila-Smirnow D, Carlier RY. WB-MRI muscle study group. Whole body muscle MRI protocol: pattern recognition in early onset NM disorders. Neuromuscul Disord. 2012; 22:Suppl 2. S68–S84.42. Axelsen MB, Eshed I, Duer-Jensen A, Møller JM, Pedersen SJ, Østergaard M. Whole-body MRI assessment of disease activity and structural damage in rheumatoid arthritis: first step towards an MRI joint count. Rheumatology (Oxford). 2014; 53:845–853.43. McLaughlin PD, Ryan J, Hodnett PA, O'Halloran D, Maher MM. Quantitative whole-body MRI in familial partial lipodystrophy type 2: changes in adipose tissue distribution coincide with biochemical improvement. AJR Am J Roentgenol. 2012; 199:W602–W606.44. Fritz J, Tzaribatchev N, Claussen CD, Carrino JA, Horger MS. Chronic recurrent multifocal osteomyelitis: comparison of whole-body MR imaging with radiography and correlation with clinical and laboratory data. Radiology. 2009; 252:842–851.45. Falip C, Alison M, Boutry N, Job-Deslandre C, Cotten A, Azoulay R, et al. Chronic recurrent multifocal osteomyelitis (CRMO): a longitudinal case series review. Pediatr Radiol. 2013; 43:355–375.46. Perez-Rossello JM, Connolly SA, Newton AW, Zou KH, Kleinman PK. Whole-body MRI in suspected infant abuse. AJR Am J Roentgenol. 2010; 195:744–750.47. Cha JG, Kim DH, Kim DH, Paik SH, Park JS, Park SJ, et al. Utility of postmortem autopsy via whole-body imaging: initial observations comparing MDCT and 3.0 T MRI findings with autopsy findings. Korean J Radiol. 2010; 11:395–340.48. Ross S, Ebner L, Flach P, Brodhage R, Bolliger SA, Christe A, et al. Postmortem whole-body MRI in traumatic causes of death. AJR Am J Roentgenol. 2012; 199:1186–1192.49. Ferreira EC, Brito CC, Domingues RC, Bernardes M, Marchiori E, Gasparetto EL. Whole-body MR imaging for the evaluation of McCune-albright syndrome. J Magn Reson Imaging. 2010; 31:706–710.50. Beck C, Morbach H, Wirth C, Beer M, Girschick HJ. Whole-body MRI in the childhood form of hypophosphatasia. Rheumatol Int. 2011; 31:1315–1320.51. Rittner RE, Baumann U, Laenger F, Hartung D, Rosenthal H, Hueper K. Whole-body diffusion-weighted MRI in a case of Rosai-Dorfman disease with exclusive multifocal skeletal involvement. Skeletal Radiol. 2012; 41:709–713.52. Kumar A, Goenka AH, Choudhary A, Sahu JK, Gulati S. Disseminated cysticercosis in a child: whole-body MR diagnosis with the use of parallel imaging. Pediatr Radiol. 2010; 40:223–227.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dynamic Contrast-Enhanced MRI and Its Applications in Various Central Nervous System Diseases
- Deep Learning Applications in Perfusion MRI: Recent Advances and Current Challenges
- High field strength magnetic resonance imaging of cardiovascular diseases
- Magnetic Resonance Imaging Meets Fiber Optics: a Brief Investigation of Multimodal Studies on Fiber OpticsBased Diagnostic / Therapeutic Techniques and Magnetic Resonance Imaging
- Fast MRI in Acute Ischemic Stroke: Applications of MRI Acceleration Techniques for MR-Based Comprehensive Stroke Imaging
