Korean J Urol.
2015 Jun;56(6):473-476. 10.4111/kju.2015.56.6.473.
Intraureteral and intravenous indocyanine green to facilitate robotic partial nephroureterectomy in a patient with complete ureteral triplication
- Affiliations
-
- 1Department of Urology, Temple University School of Medicine, Philadelphia, PA, USA. daniel.eun@tuhs.temple.edu
- KMID: 2160589
- DOI: http://doi.org/10.4111/kju.2015.56.6.473
Abstract
- A patient with a complete right ureteral triplication presented with recurrent pyelonephritis and flank pain that was refractory to medical management. Evaluation showed that the atrophic upper-most renal moiety had been chronically obstructed and was associated with a dilated ureter. Intraureteral and intravenous indocyanine green (ICG) were used as real-time contrast agents intraoperatively to facilitate right robotic partial nephroureterectomy of the diseased system. Intraureteral ICG was used to accurately distinguish the pathologic ureter and associated renal pelvis from its normal counterparts. Intravenous ICG was used to assess perfusion in the right kidney and delineate the margins of diseased renal parenchyma.
MeSH Terms
-
Administration, Topical
Adult
Coloring Agents/administration & dosage
Female
Humans
Indocyanine Green/*administration & dosage
Infusions, Intravenous
Nephrectomy/*methods
Pyelonephritis/surgery
Robotic Surgical Procedures/*methods
Tomography, X-Ray Computed
Ureter/*abnormalities/radiography/*surgery
Coloring Agents
Indocyanine Green
Figure
-

Fig. 1 (A) Coronal view suggesting three ureters, each associated with own renal pelvis. (B) Coronal view showing cortical thinning and right uppermost pole.

Fig. 2 Retrograde pyelogram showing ureteral triplication.
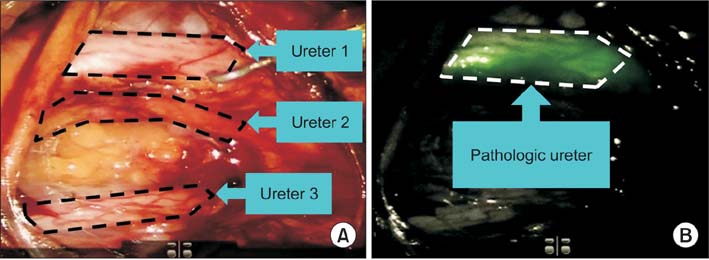
Fig. 3 (A) Three ureters visualized under white light. (B) Pathologic ureter highlighted under near-infrared fluorescence.
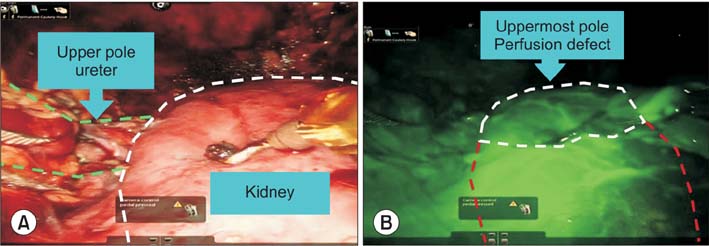
Fig. 4 (A) Kidney visualized under white light. (B) Perfusion defect delineated under near-infrared fluorescence.
Cited by 1 articles
-
Robot-assisted distal ureteral reconstruction for benign pathology: Current state
Aeen M. Asghar, Randall A. Lee, Kevin K. Yang, Michael Metro, Daniel D. Eun
Investig Clin Urol. 2020;61(Suppl 1):S23-S32. doi: 10.4111/icu.2020.61.S1.S23.
Reference
-
1. Smith I. Triplicate ureter. Br J Surg. 1946; 34:182–185.2. Sivrikaya A, Cay A, Imamoglu M, Sarihan H. A case of ureteral triplication associated with ureteropelvic junction obstruction. Int Urol Nephrol. 2007; 39:755–757.3. Lee Z, Moore B, Giusto L, Eun DD. Use of indocyanine green during robot-assisted ureteral reconstructions. Eur Urol. 2015; 67:291–298.4. Lee Z, Cadillo-Chavez R, Lee DI, Llukani E, Eun D. The technique of single stage pure robotic nephroureterectomy. J Endourol. 2013; 27:189–195.5. Hsu TH, Goldfarb DA. Blind-ending ureteral triplication. J Urol. 1998; 159:1295.6. Patel PM, Stock JA, Hanna MK, Lutzker L. Ureteral triplication with ectopic upper pole moiety. Urology. 2001; 58:279–280.7. Flechsig H, Fuchs J, Warmann SW, Schaefer JF. Magnetic resonance nephrography for planning of laparoscopic partial nephrectomy in a pediatric case of ureteral triplication. J Pediatr Surg. 2010; 45:2053–2057.8. Tobis S, Knopf J, Silvers C, Yao J, Rashid H, Wu G, et al. Near infrared fluorescence imaging with robotic assisted laparoscopic partial nephrectomy: initial clinical experience for renal cortical tumors. J Urol. 2011; 186:47–52.9. Bjurlin MA, Gan M, McClintock TR, Volpe A, Borofsky MS, Mottrie A, et al. Near-infrared fluorescence imaging: emerging applications in robotic upper urinary tract surgery. Eur Urol. 2014; 65:793–801.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Removal of Apocrinehydrocytoma Using Indocyanine Green and Sodium Hyaluronate
- A Case or Unilateral Ureteral Triplication Associated with Ipsilateral Vesicoureteral reflux
- Ablative Fractional Radiofrequency Combined with Sonophoresis Increases Skin Penetration of Indocyanine Green
- Real-time Vessel Navigation Using Indocyanine Green Fluorescence during Robotic or Laparoscopic Gastrectomy for Gastric Cancer
- Indocyanine Green Enhanced Photocoagulation in the Pigmented Rabbit
